
Blog
WGU KMM1 Task 1: Build, Buy or Lease — Pass First Try
WGU KMM1 Task 1: Service Line Development — AMT2 PRFA
The Complete Build, Buy, or Lease Guide for a First-Attempt Pass
Introduction
A hospital is a complex system of interrelated functions requiring constant movement of people and goods. Functional design of a hospital can promote skill, economy, convenience, and comfort. Nonfunctional design of a hospital can impede activities of all types, detract from quality of care, and raise costs to intolerable levels.
Healthcare facilities management examines challenging key elements, such as contracting outpatient care and quality management systems. Property development puts the focus on patient care.
In this task, you will determine whether to build, buy, or lease space for a new orthopedic service line as discussed in the “Service Line Development Case Study.”
Requirements
Your submission must represent your original work and understanding of the course material. Most performance assessment submissions are automatically scanned through the WGU similarity checker. Students are strongly encouraged to wait for the similarity report to generate after uploading their work and then review it to ensure Academic Authenticity guidelines are met before submitting the file for evaluation. See Understanding Similarity Reports for more information.
Grammarly Note:
Professional Communication will be automatically assessed through Grammarly for Education in most
performance assessments before a student submits work for evaluation. Students are strongly encouraged to review the Grammarly for Education feedback prior to submitting work for evaluation, as the overall submission will not pass without this aspect passing. See Use Grammarly for Education Effectively for more information.![]()
Microsoft Files Note:
Write your paper in Microsoft Word (.doc or .docx) unless another Microsoft product, or pdf, is specified in the task directions. Tasks may notbe submitted as cloud links, such as links to Google Docs, Google Slides, OneDrive, etc. All supporting documentation, such as screenshots and proof of experience, should be collected in a pdf file and submitted separately from the main file. For more information, please see Computer System and Technology Requirements.
You must use the rubric to direct the creation of your submission because it provides detailed criteria that will be used to evaluate your work. Each requirement below may be evaluated by more than one rubric aspect. The rubric aspect titles may contain hyperlinks to relevant portions of the course.
- Develop a business summary in which you do the following:
-
Discuss the advantages of each of the following options:
- Building space for the new orthopedic service line
- Buying space for the new orthopedic service line
- Leasing space for the new orthopedic service line
-
Discuss the disadvantages (e.g., liabilities and risks) of each of the following options:
- Building space for the new orthopedic service line
- Buying space for the new orthopedic service line
- Leasing space for the new orthopedic service line
-
Recommend what you consider to be the best option for the facility.
-
- Acknowledge sources, using in-text citations and references, for content that is quoted, paraphrased, or summarized.
- Demonstrate professional communication in the content and presentation of your submission.
WEB LINKS
Service Line Development – General Case Scenario Service Line Development – Task 1 Artifacts
Step-by-Step Guide
Introduction: Why Most Students Struggle With KMM1 Task 1
KMM1 Task 1 is one of the most misunderstood performance assessments in WGU’s AMT2 Service Line Development course. On the surface it looks straightforward — discuss the advantages and disadvantages of building, buying, or leasing space for a new orthopedic service line, then make a recommendation. Students open their laptops, write a few generic pros and cons, and hit submit expecting a pass.
Then the evaluation comes back: “Approaching Competence.” Every year, thousands of WGU healthcare management students hit this wall on Task 1, not because the assignment is conceptually difficult, but because they underestimate what “sufficient detail” actually means to a WGU evaluator — and because they fail to use the case study documents the way the rubric demands.
This guide solves that problem. It walks through the entire task — the rubric, the Trinity Community Hospital case facts, the financial analysis, the content requirements for each of the six advantage/disadvantage sections, and a recommendation framework — so that you can write a paper that meets every rubric criterion on the first attempt.
| Who this is for: WGU students currently enrolled in AMT2 Service Line Development who are preparing to submit KMM1 Task 1, or who need to revise a returned submission. No prior knowledge of real estate or facilities management is required. |
Section 1: What KMM1 Task 1 Is Really Asking
1.1 The Two Competencies Being Assessed
KMM1 Task 1 tests two competencies simultaneously. Facilities Management (705.3.3) asks whether you can effectively evaluate construction and property options for a healthcare organization. Negotiation (705.3.7) asks whether you can analyze contract structures — including lease terms — to assess financial risk and liability. Both show up in the rubric, and both require that you go beyond surface-level pros and cons.
1.2 The Deliverable: A Business Summary, Not an Academic Essay
The task calls for a “business summary.” This distinction matters. A business summary is a professional document written for a healthcare executive audience, not a five-paragraph college essay. It should be organized around the decision at hand, use precise financial language, and make a clear recommendation supported by evidence. Students who write in a casual or meandering style — or who write an academic abstract — consistently score lower on the professional communication criterion (Rubric Section C).
1.3 The Rubric at a Glance
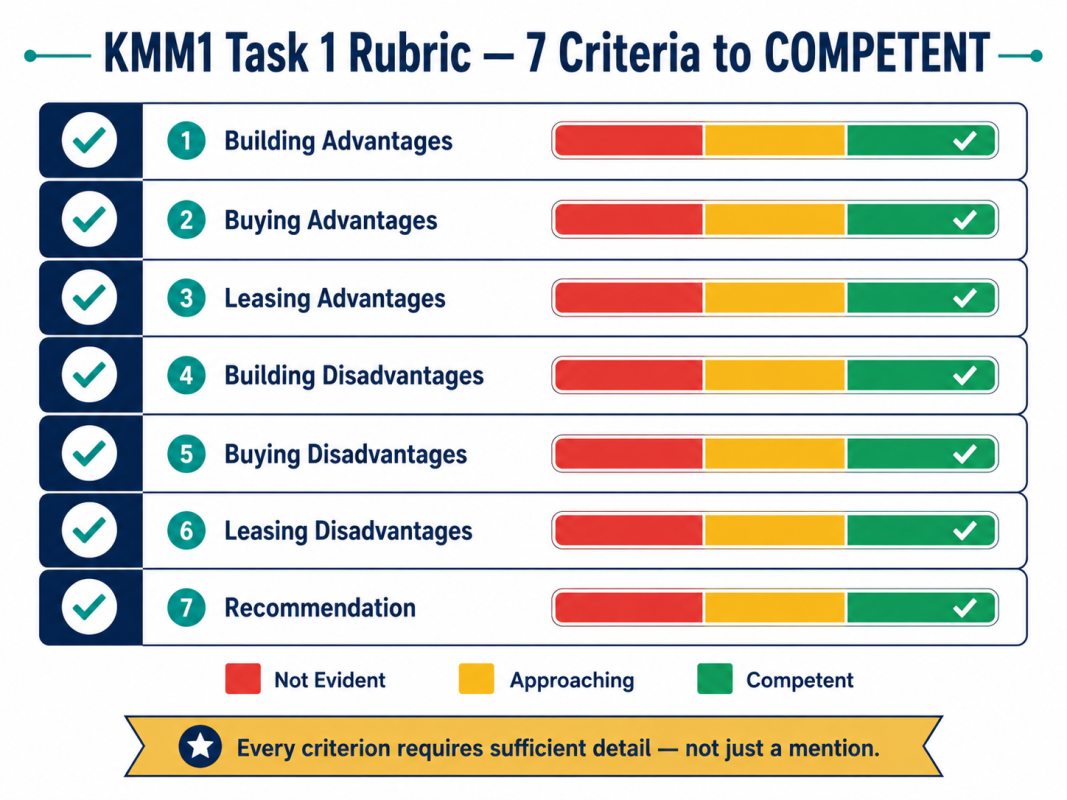
The rubric has seven graded aspects. Each requires a “logical discussion with sufficient detail” to reach COMPETENT. Reaching only “Approaching Competence” on any single aspect can cause the entire task to be returned. Here is what each aspect demands:
| Rubric Aspect | Minimum to Reach COMPETENT |
|---|---|
| A1a — Building Advantages | 3+ specific, case-grounded advantages of building space for the orthopedic service line |
| A1b — Buying Advantages | 3+ specific, case-grounded advantages of purchasing the adjacent building |
| A1c — Leasing Advantages | 3+ specific, case-grounded advantages of leasing the adjacent MOB |
| A2a — Building Disadvantages | 3+ specific disadvantages including campus space constraints and capital cost |
| A2b — Buying Disadvantages | 3+ specific disadvantages including capital reserve risk and off-campus liability concerns |
| A2c — Leasing Disadvantages | 3+ specific disadvantages; the triple net lease structure must be explicitly addressed |
| A3 — Recommendation | One clear choice with 3+ evidence-based supporting arguments tied to the case study |
| Key insight: The rubric does NOT specify which option you must recommend. Building, buying, and leasing are all defensible. What matters is the quality of the argument, not the conclusion. Students who spend their energy trying to guess “the right answer” miss the point — the evaluator rewards analysis and evidence. |
Section 2: Understanding the Trinity Community Hospital Case Study
KMM1 Task 1 is entirely grounded in the “Service Line Development Case Study” provided by WGU. Students who write generic papers — applicable to any hospital anywhere — fail to demonstrate the case-specific analysis the rubric requires. Before writing anything, you need to thoroughly understand these case facts.
2.1 Hospital Profile
Trinity Community Hospital is a 150-bed, not-for-profit facility located in the southeast United States. It operates on a 25-acre campus accessible from all major roadways and currently offers internal medicine, pulmonary medicine, gastroenterology, urology, general surgery, and several other specialties. It has 20 operating rooms and an emergency department. Support services including laboratory, radiology (two CT scanners, one MRI), pharmacy, physical therapy, and respiratory therapy are in place (Trinity Community Hospital, 2013).
The hospital has no formal oncology, orthopedic, or cardiology programs, though a few orthopedic surgeons and cardiologists hold privileges. Its strategic plan targets the development of all three service lines. This context matters for Task 1: the orthopedic PT/rehab center is one component of a larger three-program expansion, not an isolated project.
2.2 The Financial Picture
Trinity’s financial situation is the most important context for the facilities decision. The hospital has experienced three consecutive years of declining utilization and revenue. In the current year, it posted an operating loss of $1,495,000 — the first in its history. A capital reserve of approximately $25,000,000 exists, but much of it must fund the oncology center ($8,000,000), the orthopedic PT center and MRI expansion ($3,600,000), and the cardiovascular cath labs ($5,000,000) — a combined capital demand of roughly $16,600,000 (Briscoe, 2010; Trinity Community Hospital, 2013).
The CFO, Mike Corrigan, explicitly flags two concerns in the Task 1 artifact email: the hospital is running out of space to expand on campus, and maintaining an adequate capital reserve is essential if all three service lines are to be launched simultaneously (Corrigan, 2010). Every financial argument in your paper should connect back to this constraint.
2.3 The Three Options — Exact Numbers
The CFO email provides the specific figures that anchor the financial analysis. These are the numbers you must use — do not estimate or substitute:
| Option | Key Financial Details from CFO Email (Corrigan, 2010) |
|---|---|
| Build (on campus) | $120/sq ft × 5,000 sq ft = $600,000 total construction cost; 20-year depreciable life |
| Buy (adjacent building) | $700,000 total ($575,000 building + $125,000 lot); 20-year depreciable life |
| Lease (adjacent MOB) | $20/sq ft × 5,000 sq ft = $100,000/year; triple net lease structure; renovations included in rate |
| Critical detail: The lease is explicitly a triple net lease. This means Trinity would be responsible not only for the $100,000 annual rent but also for property taxes, building insurance, and all repair and maintenance costs. Many students describe the lease as the “cheapest” option without accounting for these additional obligations — a gap that evaluators consistently flag. |
2.4 Campus Space Reality
The campus hosts four medical office buildings (MOBs), each with 60,000 square feet, most leased to private physician groups. MOB 1 has 15,000 square feet of vacant space suitable for oncology. The campus can accommodate one additional MOB of up to 60,000 square feet, but space is becoming constrained. A 5,000-square-foot PT center built on campus would consume part of the remaining expansion footprint. This is a genuine disadvantage of the building option that must be addressed explicitly in Section A2a of your paper (Trinity Community Hospital, 2013).
Section 3: Advantages — What to Write and How to Write It
This is the section where most papers earn “Approaching Competence” rather than “Competent.” The failure mode is almost always the same: the student lists one or two generic advantages per option without connecting them to Trinity’s specific situation. The fix is equally consistent: for each advantage, name it, explain the mechanism, and connect it to a specific Trinity fact or constraint.
3.1 Building Advantages (Rubric A1a)
Advantage 1: On-Campus Integration and Operational Synergies
Constructing the PT/rehab center on Trinity’s existing campus places it immediately adjacent to the emergency department, operating suites, radiology (including the MRI scanners critical for orthopedic diagnosis), pharmacy, and dietary services. These departments are already staffed and operational. When a post-surgical orthopedic patient transitions to physical therapy, the care pathway is seamless — no transport logistics, no duplicate admission processes, no separate facility navigation. More importantly, Trinity would not need to hire additional housekeeping, facilities maintenance, or support staff for the new building because those services already cover the campus. This operational integration directly reduces the incremental cost of running the service line (Shohet & Lavy, 2004).
Advantage 2: Full Design Customization
Unlike buying an existing structure or leasing an MOB, ground-up construction allows Trinity’s clinical leadership to design the PT/rehab center from scratch around orthopedic workflow requirements. Equipment placement, ceiling heights for gait training and parallel bars, private treatment rooms, ADA accessibility features, and proximity to the elevator bank connecting to surgical floors can all be engineered in from day one. A building designed for orthopedic rehabilitation will outperform a repurposed medical office in patient outcomes and staff efficiency (White & Griffith, 2019).
Advantage 3: Long-Term Asset and Tax Advantages
The CFO’s email confirms a 20-year depreciable life for the constructed building (Corrigan, 2010). Depreciation generates an annual non-cash tax deduction that reduces Trinity’s net cost of ownership over time. As a not-for-profit hospital, Trinity also benefits from potential property tax exemptions on hospital-owned real estate in most southeastern states. Additionally, owned real estate builds equity — a financial asset that can be leveraged for future capital needs, refinanced, or, if the service line is eventually consolidated, sold.
Advantage 4: Brand Visibility and Patient Wayfinding
Trinity’s strategic plan identifies market differentiation as a core objective — it aims to become the regional premier provider of orthopedic care. A new, purpose-built facility on Trinity’s recognizable campus reinforces that brand identity. Patients and referring physicians do not need to be given directions to an off-campus location; the building is visible from major roadways alongside the main hospital. This eliminates one of the most documented barriers to new service line adoption: patients who never find the facility on their first visit (Berkowitz, 2017).
3.2 Buying Advantages (Rubric A1b)
Advantage 1: Faster Time to Revenue Than Building
Construction timelines in healthcare typically run 12 to 24 months from groundbreaking to occupancy, depending on permitting, contractor availability, and inspection cycles. Purchasing the adjacent building eliminates the construction phase entirely. After closing and completing targeted renovations — which the CFO notes are already partially accounted for in the financial modeling — the PT center could open in weeks to months rather than over a year. Given Trinity’s three-year revenue decline and operating loss, accelerating the orthopedic program’s revenue generation timeline directly addresses the hospital’s most urgent financial problem (Zelman et al., 2020).
Advantage 2: Campus Expansion Without On-Site Space Consumption
The CFO explicitly notes that Trinity is running out of space on its 25-acre campus (Corrigan, 2010). Purchasing the adjacent building for the orthopedic PT center relocates that program off-campus while preserving the remaining on-site footprint for a service line that requires hospital infrastructure — most notably the cardiovascular program, which needs proximity to the cardiac care unit and operating rooms for its cath lab procedures. Buying satisfies orthopedic space needs without foreclosing future on-campus development options.
Advantage 3: Asset Appreciation and Equity
Real estate in a growing southeastern market — the case study notes 4% annual population growth and continued high-tech industry expansion in the region — tends to appreciate over time. Purchasing the adjacent building at $700,000 today secures the asset at current market value. Over a 20-year depreciable life, Trinity builds equity in the property while benefiting from tax depreciation. Should the orthopedic service line eventually be consolidated or relocated, the building retains resale value (Shohet & Lavy, 2004).
Advantage 4: Adjacent Vacant Lot for Future Expansion
The $125,000 lot included in the purchase price provides future expansion space for the orthopedic program without requiring a second property acquisition. As orthopedic case volumes scale toward the strategic plan’s 5-year target of 2,100 surgical cases and 6,500 physical therapy visits annually, Trinity may need to expand the PT center’s square footage. Owning the adjacent lot makes that expansion possible without re-entering the real estate market (Trinity Community Hospital, 2013).
3.3 Leasing Advantages (Rubric A1c)
Advantage 1: Capital Preservation for a Multi-Program Expansion
Leasing requires no upfront purchase price. At $100,000 per year, the lease preserves $600,000 to $700,000 in capital that would otherwise be consumed by building or buying. Against a backdrop of three simultaneous service line launches — orthopedic, oncology ($8M), and cardiovascular ($5M) — capital preservation is not merely a preference but a strategic necessity. The CFO’s note about maintaining an adequate capital reserve directly supports this framing (Corrigan, 2010).
Advantage 2: Fastest Path to Opening
The lease rate of $20 per square foot includes necessary renovations to prepare the MOB space for physical therapy and rehab use. No construction timeline, no acquisition closing process, no permitting delay for ground-up construction. The PT center can open and begin generating physical therapy visit revenue more quickly under the lease option than under either the build or buy scenarios. Given that each month of delay represents lost revenue during Trinity’s financial recovery, speed carries real dollar value.
Advantage 3: Reduced Financial Risk for an Unproven Program
Trinity has no formal orthopedic program today. The 5-year target of 2,100 surgical cases and 6,500 PT visits represents a projection, not a guarantee. If the program fails to achieve projected volumes — a real risk given two well-established competitors with strong orthopedic programs located seven and ten miles away — Trinity’s financial exposure is bounded by the annual lease cost rather than a $600,000 to $700,000 capital write-down. Leasing functions as a risk management strategy appropriate to a hospital in operating-loss territory entering a new specialty (Zelman et al., 2020).
Advantage 4: Flexibility to Pivot
If the orthopedic service line evolves in ways not currently anticipated — physician group affiliations change, competitor dynamics shift, the program merges with the cardiovascular or oncology centers — a lease provides the flexibility to renegotiate terms, relocate, or discontinue the arrangement in ways that ownership does not. Strategic flexibility has financial value in a volatile healthcare market (White & Griffith, 2019).
Section 4: Disadvantages and Risks — The Liabilities You Must Address
The rubric specifically uses the language “disadvantages (e.g., liabilities and risks).” This means you are expected to go beyond inconvenience-level observations and address genuine financial, operational, and contractual risks. This is the section that most separates passing papers from those returned for revision.
4.1 Building Disadvantages (Rubric A2a)
Disadvantage 1: Highest Capital Cost and Capital Reserve Drain
At $600,000, on-campus construction represents the single largest upfront capital commitment of the three options. Given that Trinity must simultaneously fund the oncology center ($8M), cardiovascular cath labs ($5M), and an MRI expansion ($3M), the building option places the greatest strain on the $25M capital reserve. If construction costs overrun — a common occurrence in healthcare facility projects — the reserve exposure increases further (Zelman et al., 2020).
Disadvantage 2: Longest Timeline to Revenue
Healthcare construction typically requires 12 to 24 months from design approval to occupancy. During that period, Trinity earns no revenue from orthopedic physical therapy visits, which represent a projected $1,787,500 in gross charges annually at the 5-year target volume. Every month of construction delay is a month of lost revenue during a period when Trinity is already in operating loss. No other option imposes this timeline penalty (Briscoe, 2010).
Disadvantage 3: Campus Space Consumption
Building a 5,000-square-foot structure on campus consumes scarce remaining expansion capacity. The CFO notes that Trinity is running out of on-site space (Corrigan, 2010). Allocating that space to the orthopedic PT center forecloses its availability for a future service that requires more direct hospital connectivity — such as a cardiac step-down unit or a surgical oncology suite. This is a strategic opportunity cost, not just a real estate constraint.
Disadvantage 4: Construction Risk and Operational Disruption
Active construction adjacent to an operating hospital creates patient experience challenges, infection control considerations, and noise management obligations. Healthcare facility construction also carries inherent cost and schedule risk — supply chain delays, contractor performance issues, and regulatory inspections can all extend timelines and budgets beyond initial projections.
4.2 Buying Disadvantages (Rubric A2b)
Disadvantage 1: Highest Total Cost
At $700,000 ($575,000 building plus $125,000 lot), purchasing the adjacent building is the most expensive option in terms of upfront capital outlay. For a hospital operating at a loss with a capital reserve that must fund three simultaneous service lines, the $100,000 premium over the building option and $600,000 premium over annual lease cost represents material financial risk (Corrigan, 2010).
Disadvantage 2: Long-Term Liability and Ownership Obligations
Property ownership creates permanent financial obligations that persist regardless of whether the orthopedic service line succeeds. Property taxes, liability insurance, facility maintenance, systems replacement, and eventual capital reinvestment become Trinity’s responsibility in perpetuity. If the service line underperforms or Trinity’s strategic priorities shift, the hospital holds a building it must continue to maintain or dispose of — neither of which is cost-free (Shohet & Lavy, 2004).
Disadvantage 3: Off-Campus Access and Reimbursement Challenges
Moving the PT center off-campus introduces patient navigation challenges. Physical therapy patients, many of them post-surgical with limited mobility, must travel to and locate a separate facility — increasing the likelihood of missed appointments, dissatisfaction, and early program abandonment. From a reimbursement perspective, services delivered in a non-hospital-based outpatient setting typically receive lower CMS and commercial insurance rates than hospital-based departments, directly reducing revenue per visit (White & Griffith, 2019).
4.3 Leasing Disadvantages (Rubric A2c)
Disadvantage 1: Triple Net Lease — True Cost Significantly Exceeds Base Rent
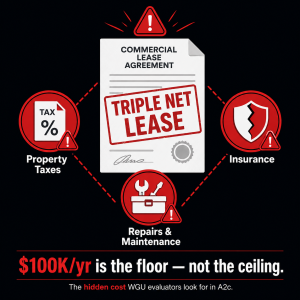
The lease is structured as a triple net (NNN) lease, a commercial real estate arrangement in which the tenant — Trinity — is responsible for property taxes, building insurance, and all maintenance and repair costs in addition to base rent (Corrigan, 2010). Under a standard triple net lease, these costs typically add 15% to 30% to the base rent, meaning Trinity’s true annual occupancy cost could approach $115,000 to $130,000 or more. Furthermore, if the building requires major system repairs — HVAC, roofing, plumbing — Trinity bears those costs in full. The “$100,000/year” figure is a floor, not a ceiling (Senn, 2020).
Disadvantage 2: No Equity, No Asset Value
Every dollar paid in lease costs is an operating expense. Unlike owning, Trinity accumulates no equity, builds no asset on its balance sheet, and gains no appreciating property value. Over a 20-year horizon equivalent to the depreciable life of a purchased or constructed building, Trinity would pay $2,000,000 in base rent alone — with nothing to show on its asset register at the end. Ownership converts those payments into a capital asset; leasing does not.
Disadvantage 3: No Depreciation Tax Benefit
The Internal Revenue Code allows healthcare organizations to depreciate owned real property over its useful life, generating an annual non-cash deduction that reduces taxable income. Even as a not-for-profit, Trinity can use this mechanism for unrelated business income. Leased property generates no depreciation deduction, eliminating this financial advantage entirely (Zelman et al., 2020).
Disadvantage 4: Relocation Risk at Lease Expiration
When the lease term ends, the landlord may decline renewal, demand materially higher rent, or sell the property to a third party. At that point, Trinity faces the choice of relocating an established orthopedic PT program — with all the patient disruption, marketing costs, and operational overhead that entails — or accepting whatever terms the landlord demands. This uncertainty represents a strategic liability that builds as the program matures and relocation becomes more disruptive (White & Griffith, 2019).
Disadvantage 5: Limited Renovation and Customization Rights
Although the lease rate includes “necessary renovations,” Trinity cannot make structural modifications or capital improvements to a building it does not own without landlord consent. Future equipment upgrades, ADA modifications, or workflow redesigns may require negotiation and may be denied. Over time, this limitation can constrain the program’s clinical development.
Section 5: Writing a Winning Recommendation (Rubric A3)
The recommendation section is where the most points are lost. A passing recommendation is not a restatement of the advantages. It is a synthesis — a structured argument that explains why the chosen option is superior given Trinity’s specific financial, strategic, and operational context. It should also briefly acknowledge why the other two options were set aside.
Both the lease and the build options are highly defensible in this case study, and different evaluators have accepted both. Below is a complete recommendation argument for the lease option, followed by a note on how to argue for building or buying.
5.1 Sample Recommendation: Lease (Argument Structure)
Opening Statement
Based on the analysis above, leasing the adjacent medical office building is recommended as the best option for Trinity Community Hospital’s orthopedic PT/rehab center at this time. This recommendation is grounded in Trinity’s current financial constraints, the strategic priority of capital preservation across all three service line investments, and the need to generate revenue quickly during a period of operating loss.
Argument 1 — Capital Stewardship Across Three Service Lines
Trinity’s strategic plan commits the hospital to developing oncology ($8M), orthopedic ($3.6M+), and cardiovascular ($5M) programs simultaneously from a $25M capital reserve — a reserve that is already under pressure from an operating loss. The lease option retains $600,000 to $700,000 in capital that the build or buy options would immediately consume. That preserved capital can fund oncology infusion suite renovations or cardiovascular cath lab equipment without additional borrowing, directly supporting Trinity’s goal of profitability-driven growth (Corrigan, 2010; Briscoe, 2010).
Argument 2 — Fastest Path to Revenue During a Financial Recovery
With renovations included in the $20/sq ft lease rate, the PT center can be open and generating physical therapy visits within weeks of lease execution — not the 12 to 24 months a construction project would require. At a projected 6,500 physical therapy visits annually and a gross charge of $275/visit, the orthopedic program is projected to generate $1,787,500 in gross PT revenue per year. Every month of delay costs Trinity approximately $149,000 in gross charges. Leasing minimizes that delay (Briscoe, 2010).
Argument 3 — Risk Proportionate to an Unproven Program
Trinity has no established orthopedic program. The projected 2,100 surgical cases represent aspirational volume in a competitive market where both Tertiary Medical Center and Regional Hospital already offer strong orthopedic services. Leasing limits Trinity’s downside exposure to annual rent costs rather than a stranded capital asset should volumes disappoint. This risk profile is appropriate for a hospital launching a new specialty in an already-competitive market (Zelman et al., 2020; White & Griffith, 2019).
Why Not Build or Buy?
Building offers superior long-term asset value and operational integration but imposes the longest revenue delay and the second-highest capital cost — both misaligned with Trinity’s immediate financial recovery needs. Buying is faster than building but carries the highest upfront cost ($700,000), permanent ownership liability, and the off-campus access and reimbursement rate disadvantages. Neither option is wrong in principle; both are simply less well-matched to Trinity’s current risk tolerance and capital position than leasing.
| Note on recommending build or buy: If you prefer to recommend building, anchor the argument on: on-campus integration reducing operating overhead, the long-term asset value outweighing short-term capital cost, and Trinity’s strategic goal of becoming the regional orthopedic center (which benefits from co-location). If recommending buying, emphasize speed vs. building, the adjacent lot for future expansion, and campus space preservation. |
Section 6: APA 7 Citations — What to Cite and How
Rubric Section B requires in-text citations AND a reference list for all quoted, paraphrased, or summarized content. This is one of the easiest rubric sections to pass — and one of the most commonly failed due to omission. Use the following citation structure.
6.1 In-Text Citations for Case Study Documents
- CFO email — cite whenever referencing construction costs, purchase price, lease rate, depreciable life, or the capital reserve note: (Corrigan, 2010)
- Fact Sheet — cite for hospital profile, campus facts, utilization data, financial trends, and competitive environment: (Trinity Community Hospital, 2013)
- Strategic Plan — cite for 5-year targets, capital investment figures, mission/vision statements, and program goals: (Briscoe, 2010)
6.2 Reference List Entries (APA 7, Hanging Indent)
Include all case study sources plus any peer-reviewed support you add. Verified entries:
Berkowitz, E. N. (2017). Essentials of health care marketing (4th ed.). Jones & Bartlett Learning.
Briscoe, M. (2010). Five-year program plan [PowerPoint presentation]. Trinity Community Hospital Strategic Planning Department.
Corrigan, M. (2010). Info for build/buy/lease [Internal memorandum to CEO Morgan Reece]. Trinity Community Hospital.
Senn, M. (2020). Commercial real estate analysis and investments (3rd ed.). CCIM Institute.
Shohet, I. M., & Lavy, S. (2004). Healthcare facilities management: State of the art review. Facilities, 22(7/8), 210–220. https://doi.org/10.1108/02632770410527570
Trinity Community Hospital. (2013). Trinity Community Hospital fact sheet. Western Governors University, AMT2 Service Line Development Case Study.
White, K. R., & Griffith, J. R. (2019). The well-managed healthcare organization (9th ed.). Health Administration Press.
Zelman, W. N., McCue, M. J., & Glick, N. D. (2020). Financial management of health care organizations: An introduction to fundamental tools, concepts, and applications (5th ed.). Wiley-Blackwell.
Section 7: Formatting Requirements That Affect Your Score
WGU evaluators assess professional communication (Rubric Section C) based partly on Grammarly for Education scores and partly on formatting consistency. Papers with formatting errors do not automatically fail, but they signal carelessness and can reinforce an “Approaching Competence” rating on Section C when combined with writing quality issues.
| Formatting Element | Correct Specification |
|---|---|
| Font | Times New Roman, 12pt throughout |
| Line spacing | Double-spaced throughout, including references |
| Margins | 1 inch on all four sides |
| Page size | US Letter (8.5 × 11 inches) — not A4 |
| File format | .doc or .docx — NOT Google Docs, PDF, or cloud link |
| Title page | Paper title, your name, course code (AMT2/KMM1), submission date |
| Abstract | NOT required — do not include one |
| References page | New page at end; centered “References” heading; APA 7 hanging indent |
| Headers/subheadings | Use them — they organize the paper around rubric sections |
| Length | 1,200–1,800 words is appropriate; longer is fine if content is substantive |

Section 8: Pre-Submission Checklist
Complete every item on this list before uploading to the WGU assessment portal:
- Paper is in .doc or .docx format (not a cloud link, not a PDF)
- Title page includes paper title, name, course code (AMT2/KMM1), and date
- Times New Roman 12pt, double-spaced, 1-inch margins throughout
- No abstract included
- Introduction contextualizes Trinity Community Hospital and introduces the three options
- Section A1a: 3+ building advantages grounded in Trinity’s campus setup, CFO data, and strategic goals
- Section A1b: 3+ buying advantages referencing case-specific financials and expansion context
- Section A1c: 3+ leasing advantages including capital preservation and speed-to-open arguments
- Section A2a: 3+ building disadvantages including campus space constraints, timeline, and capital cost
- Section A2b: 3+ buying disadvantages including capital reserve risk, off-campus access, and reimbursement
- Section A2c: 3+ leasing disadvantages — triple net lease structure explicitly defined and analyzed
- Exact financial figures used: build = $600K; buy = $700K; lease = $100K/yr
- Section A3: Clear recommendation named; 3+ evidence-based supporting arguments; other options acknowledged
- CFO email (Corrigan, 2010) cited at least once
- In-text citations present for all paraphrased or summarized case facts
- References page on a new page; APA 7 format; all cited sources listed
- Paper submitted through Grammarly for Education; no major Correctness errors remain
- Similarity report reviewed; no extended passages matching previously submitted student work
Section 9: Frequently Asked Questions
Is there a “right” answer for the recommendation?
No. WGU evaluators are trained to assess the quality of the argument, not whether you chose build, buy, or lease. All three options have been recommended in passing papers. What matters is that your recommendation is specific, supported by at least three evidence-based reasons tied to the case study, and acknowledges why the other options were not selected.
How long does the paper need to be?
The rubric does not specify a minimum word count for Task 1. Based on rubric requirements alone — three detailed advantages and disadvantages per option plus a supported recommendation — a well-executed paper will typically run 1,200 to 1,800 words plus references. Writing more is fine if the content is substantive; writing less risks “insufficient detail” citations from the evaluator.
Do I need peer-reviewed sources?
The rubric requires you to acknowledge sources for content that is “quoted, paraphrased, or summarized” — this language covers the case study documents. Peer-reviewed sources are not explicitly required for Task 1. However, adding one or two healthcare management or real estate references strengthens the scholarly quality of the paper and can support broader claims about industry norms (e.g., reimbursement rate differences for on- vs. off-campus facilities).
What is a triple net lease and why does it matter so much?
A triple net (NNN) lease is a commercial real estate arrangement in which the tenant pays base rent plus all three major building operating expenses: property taxes, building insurance, and maintenance/repair costs. In a standard gross lease, those costs are the landlord’s responsibility. In Trinity’s case, the $100,000 annual lease is NNN, meaning Trinity’s true occupancy cost is higher — potentially $115,000 to $130,000 or more depending on the building’s condition and tax assessment. Evaluators specifically look for this distinction in Section A2c. Papers that describe the lease simply as “$100,000 per year” without addressing the NNN structure are typically returned as Approaching Competence.
Can I write this task without reading the case study documents?
Technically possible; practically, no. Papers that do not reference specific figures from the CFO email, specific campus facts from the Fact Sheet, or specific strategic targets from the Strategic Plan consistently receive “Approaching Competence” for lacking sufficient case-specific detail. The documents are provided for a reason. Read the CFO email especially — it contains the financial data that grounds every section of this paper.
Conclusion
KMM1 Task 1 is a fair, straightforward assessment once you understand what it is actually testing. It is not asking you to know commercial real estate or healthcare construction inside and out. It is asking you to read the case study documents, understand Trinity Community Hospital’s financial and strategic situation, and apply that context to a three-option facilities decision in a professional, well-organized business summary.
The students who receive “Approaching Competence” are almost always students who wrote generically, skipped the CFO email, underexplained the triple net lease, or submitted a one-paragraph recommendation. The students who pass on the first attempt write specifically — they name the $600,000 build cost, they explain why the capital reserve constraint matters, they tell the evaluator what a triple net lease actually costs Trinity, and they defend a recommendation with three concrete arguments.
That is the entire gap. This guide has given you everything you need to close it. Use the outline in Section 3–5, verify your numbers against the CFO email, run through the checklist in Section 8, and submit with confidence.
References
- Berkowitz, E. N. (2017). Essentials of health care marketing (4th ed.). Jones & Bartlett Learning.
- Briscoe, M. (2010). Five-year program plan [PowerPoint presentation]. Trinity Community Hospital Strategic Planning Department.
- Corrigan, M. (2010). Info for build/buy/lease [Internal memorandum to CEO Morgan Reece]. Trinity Community Hospital.
- Senn, M. (2020). Commercial real estate analysis and investments (3rd ed.). CCIM Institute.
- Shohet, I. M., & Lavy, S. (2004). Healthcare facilities management: State of the art review. Facilities, 22(7/8), 210–220. https://doi.org/10.1108/02632770410527570
- Trinity Community Hospital. (2013). Trinity Community Hospital fact sheet. Western Governors University, AMT2 Service Line Development Case Study.
- Western Governors University. (n.d.). KMM1 task 1: Service line development — AMT2. WGU eLearning Platform.
- White, K. R., & Griffith, J. R. (2019). The well-managed healthcare organization (9th ed.). Health Administration Press.
- Zelman, W. N., McCue, M. J., & Glick, N. D. (2020). Financial management of health care organizations: An introduction to fundamental tools, concepts, and applications (5th ed.). Wiley-Blackwell.