
Blog
Step-by-Step Guide: Psychopharmacology Scavenger Hunt Concept Map

Psychopharmacology Scavenger Hunt Concept Map
1. Overview: Purpose of This Assignment
In psychopharmacology, understanding how medications interact with receptors at a mechanistic level is foundational to clinical practice. This assignment — the Psychopharmacology Scavenger Hunt Concept Map — asks students to map eight real-world psychiatric medications onto the four positions of the agonist spectrum, explain their mechanisms of action, identify targeted receptors, and describe the role of the cytochrome P450 enzyme system in pharmacokinetics.
This guidance typically covers three things:
- A clear, accurate explanation of agonist spectrum theory (agonist, partial agonist, antagonist, inverse agonist)
- Correct, evidence-based classification of the eight listed drugs
- A usable, visually organized framework that you can adapt into your own concept map
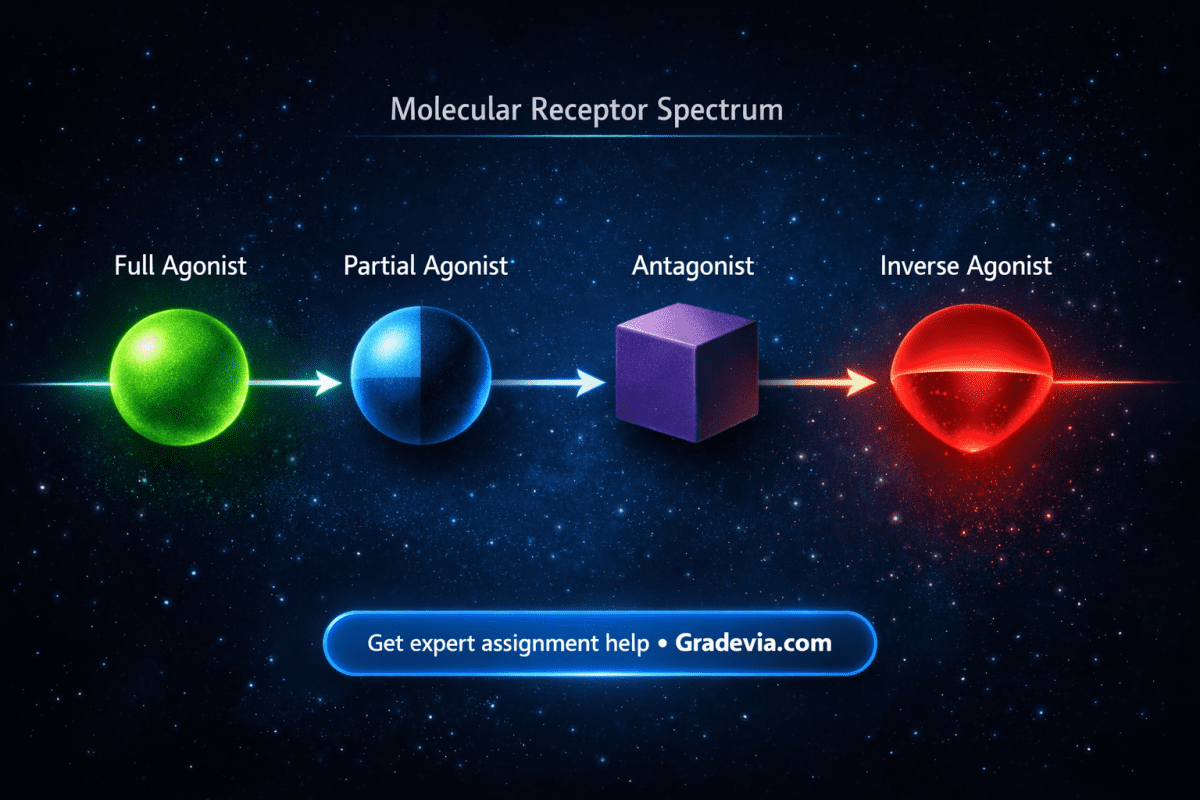
2. The Agonist Spectrum: Core Theory
Receptors are proteins that detect chemical signals. A ligand (drug or neurotransmitter) binds to the receptor and produces a response — or blocks one. The agonist spectrum describes the range of possible receptor responses based on the nature of the ligand.
| FULL AGONIST | PARTIAL AGONIST | ANTAGONIST | INVERSE AGONIST |
| 100% receptor activation | Partial activation (<100%) | Blocks endogenous ligand; no intrinsic activity | Suppresses baseline activity below normal |
2a. Full Agonist
A full agonist binds to a receptor and activates it to its maximum possible response — equivalent to the endogenous ligand at the same concentration. This produces full intrinsic activity (efficacy = 1.0). The magnitude of the response is dose-dependent up to the ceiling effect of receptor saturation.
- Mechanism: Binding stabilizes the receptor in its active conformation, triggering intracellular signaling cascades (e.g., G-protein activation, ion channel opening, second messenger production).
- Key example: Morphine and oxycodone at mu-opioid receptors produce full agonist effects — maximal analgesia, respiratory depression, and euphoria.
- Clinical relevance: High efficacy makes full agonists powerful but increases abuse potential and side effect burden.
2b. Partial Agonist
A partial agonist binds to the same receptor as a full agonist but produces a submaximal response even at full receptor occupancy. Its intrinsic efficacy falls between 0 and 1. This dual nature creates a ceiling effect that is therapeutically advantageous in many psychiatric settings.
- Mechanism: The partial agonist stabilizes an intermediate receptor conformation — more active than resting but less than fully activated. When the endogenous agonist is absent, the drug stimulates the receptor; when endogenous agonist levels are high, the drug competes and net receptor activation is reduced.
- This is called functional antagonism in high-agonist environments and functional agonism in low-agonist environments.
- Key examples: Aripiprazole (D2/D3 dopamine receptors) and brexpiprazole (D2 receptors) — both used in schizophrenia and as antidepressant adjuncts.
- Clinical relevance: Stabilizes neurotransmission by “buffering” receptor activity. Lower risk of causing full agonist toxicity.
2c. Antagonist
An antagonist binds to a receptor but produces no intrinsic activation (efficacy = 0). Its therapeutic action comes exclusively from blocking the endogenous ligand or other agonists from accessing the receptor. Antagonists are broadly divided into competitive (reversible) and non-competitive (often irreversible) categories.
- Competitive antagonist: Binds the same orthosteric site as the agonist. Increasing agonist concentration can overcome the block — the dose-response curve shifts rightward.
- Non-competitive antagonist: Binds an allosteric site or irreversibly binds the orthosteric site. Cannot be overcome by increasing agonist concentration.
- Key examples: Haloperidol (D2 receptor antagonist in antipsychosis), naloxone (mu-opioid antagonist used in opioid overdose reversal), risperidone (D2 and 5-HT2A antagonist).
- Clinical relevance: Blocking overactive dopamine in psychosis reduces positive symptoms. Blocking mu-opioid receptors rapidly reverses opioid-induced respiratory depression.
2d. Inverse Agonist
An inverse agonist binds to the same receptor site as an agonist but produces the opposite effect. Receptors exist in dynamic equilibrium between active and inactive states even without a ligand present. This baseline activity is called constitutive activity. Inverse agonists preferentially bind and stabilize the inactive conformation, reducing receptor activity below baseline.
- Mechanism: Shifts the active-inactive equilibrium toward the inactive state, suppressing spontaneous receptor signaling that occurs in the absence of any ligand.
- Distinction from antagonist: A pure antagonist has zero intrinsic efficacy (blocks agonist, does not change baseline). An inverse agonist has negative intrinsic efficacy (reduces signaling below basal levels).
- Key example: Pimavanserin — a selective 5-HT2A inverse agonist/antagonist approved for Parkinson’s disease psychosis. It has no dopamine receptor activity.
- Clinical relevance: Targeting constitutive receptor activity may be especially useful where baseline receptor overactivation contributes to pathology.
3. The Eight Medications: Agonist Spectrum Placement
Each of the eight medications listed in the assignment must be correctly placed on the agonist spectrum. Misclassification is the most common error and directly impacts grading. The table below provides classification, receptor target, mechanism, and clinical use.
| Medication | Spectrum Position | Primary Receptor | Mechanism of Action | Clinical Use |
| Oxycodone | Full Agonist | Mu-opioid (MOR) | Maximally activates MOR; increases K+ conductance, decreases Ca2+ conductance, reducing neuronal excitability and pain signaling. | Moderate-to-severe pain management. High abuse potential. Schedule II controlled substance. |
| Amphetamine | Full Agonist (indirect) | Dopamine, NE, 5-HT transporters (DAT, NET) | Reverses monoamine transporters, flooding the synapse with dopamine and norepinephrine. Also inhibits MAO. | ADHD, narcolepsy. Schedule II. Used therapeutically; high abuse liability. |
| Aripiprazole | Partial Agonist | D2, D3, 5-HT1A (partial); 5-HT2A (antagonist) | Partial D2 agonism stabilizes dopaminergic tone. Buffers hypo- and hyperactivation. | Schizophrenia, bipolar disorder, major depressive disorder (adjunct), irritability in autism. |
| Brexpiprazole | Partial Agonist | D2, 5-HT1A (partial); 5-HT2A, alpha-1A (antagonist) | Second-generation atypical with partial D2 agonism and serotonin modulation. Lower intrinsic activity than aripiprazole. | Schizophrenia, adjunctive MDD, agitation in Alzheimer’s disease (FDA approved 2023). |
| Haloperidol | Antagonist | D2 receptor (postsynaptic) | Competitive D2 blockade in mesolimbic pathway reduces positive symptoms. Also blocks D1, alpha-1, histamine H1. | Schizophrenia, acute psychosis, Tourette syndrome, acute agitation. High EPS risk. |
| Naloxone | Antagonist | Mu-, kappa-, delta-opioid receptors | Competitive opioid receptor antagonism. Displaces opioid agonists from receptors. Rapid onset, short half-life (30-90 min). | Emergency reversal of opioid overdose (Narcan). Also component of Suboxone. No agonist activity. |
| Risperidone | Antagonist | D2, 5-HT2A (primary); alpha-1, H1 | D2 and 5-HT2A dual antagonism. 5-HT2A blockade modulates dopamine release, reducing EPS vs. typical antipsychotics. | Schizophrenia, bipolar mania, irritability in autism. Second-generation (atypical) antipsychotic. |
| Pimavanserin | Inverse Agonist | 5-HT2A (primarily); some 5-HT2C | Selectively suppresses constitutive 5-HT2A activity. No dopamine receptor activity — avoids worsening motor symptoms. | Parkinson’s disease psychosis. First-in-class; FDA approved 2016 specifically for PD psychosis. |
Note on Amphetamine classification: Amphetamine is classified as an indirect full agonist because it does not bind the dopamine receptor directly but maximally triggers dopamine receptor activation by flooding the synapse. Some sources classify it as a “releasing agent” — both framings are acceptable if explained clearly in the concept map.
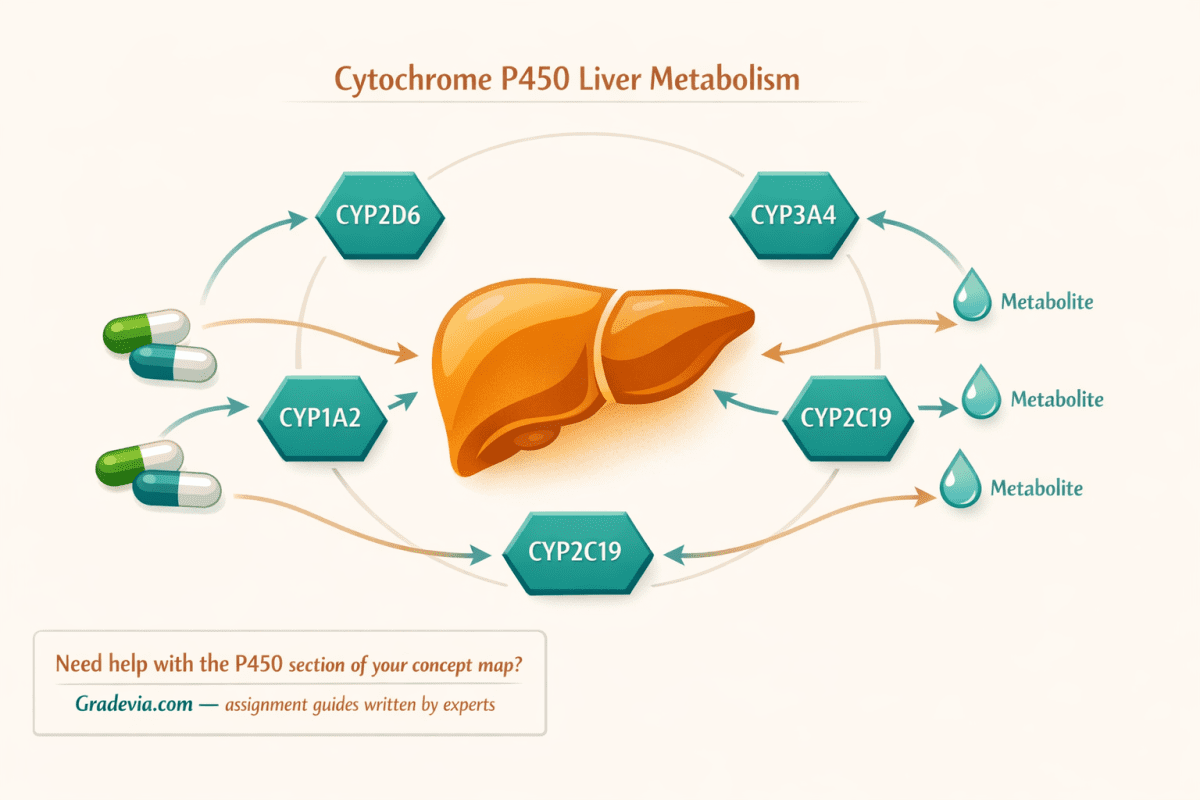
4. The Cytochrome P450 (CYP450) Enzyme System
The CYP450 enzyme system is the primary metabolic machinery for psychiatric medications. Understanding it is critical for explaining how drugs are absorbed, distributed, and cleared — as well as why drug-drug interactions, genetic polymorphisms, and individual variability affect treatment outcomes.
4a. What Is the CYP450 System?
The cytochrome P450 enzymes are a superfamily of heme-containing monooxygenase enzymes found primarily in the liver (also intestines, kidneys, lungs, and brain). They perform Phase I biotransformation — oxidative reactions that chemically modify drugs to make them more water-soluble for excretion. The resulting metabolites may be:
- Active: The metabolite retains or gains pharmacological activity (e.g., risperidone’s active metabolite paliperidone).
- Inactive: The metabolite has no pharmacological effect and is excreted.
- Toxic: Some metabolites are more harmful than the parent compound.
4b. Key CYP450 Isoforms in Psychiatry
| Enzyme | Substrates (Selected Psychiatric Drugs) | Clinical Significance |
| CYP2D6 | Aripiprazole, brexpiprazole, haloperidol, risperidone, oxycodone (partial) | Highly polymorphic. Poor metabolizers have ~10x higher drug exposure. Inhibited by fluoxetine, paroxetine. |
| CYP3A4 | Aripiprazole, brexpiprazole, oxycodone, pimavanserin, haloperidol | Most abundant hepatic CYP. Induced by carbamazepine, rifampin (reduces drug levels). Inhibited by ketoconazole, grapefruit. |
| CYP2C19 | Some benzodiazepines, tricyclics, SSRIs | Poor metabolizers common in East Asian populations. Important in antidepressant dosing. |
| CYP1A2 | Haloperidol (minor), clozapine, olanzapine | Induced by smoking. Smokers metabolize clozapine and olanzapine significantly faster. |
4c. Pharmacokinetic Role: ADME
The P450 system operates at multiple stages of pharmacokinetics:
Absorption (First-Pass Effect)
CYP3A4 and CYP2D6 in the intestinal wall and liver metabolize drugs before they reach systemic circulation. This first-pass metabolism can dramatically reduce bioavailability. Oxycodone, for example, is extensively metabolized via CYP3A4 to noroxycodone (inactive) and via CYP2D6 to oxymorphone (active, more potent).
Distribution
CYP450 activity influences the amount of free drug available for distribution. Highly protein-bound drugs compete for binding sites, and metabolic rate influences plasma concentration. Aripiprazole and brexpiprazole are both highly protein-bound (>99%) and have long half-lives partly because of slower CYP3A4/2D6 metabolism.
Clearance/Elimination
Hepatic metabolism via CYP450 enzymes converts lipophilic drugs into more hydrophilic metabolites suitable for renal or biliary excretion. Naloxone is rapidly cleared (half-life ~60-90 min) via glucuronidation (Phase II) following Phase I oxidation, necessitating repeat dosing in overdose reversal. Pimavanserin has an extended half-life (~57 hours) due to slower CYP3A4 processing.
4d. Drug-Drug Interactions (DDIs)
CYP450 interactions are clinically critical in psychiatric polypharmacy. The two mechanisms:
- Enzyme Inhibition: A drug blocks CYP metabolism of another, raising plasma levels. Example: Adding fluoxetine (CYP2D6 inhibitor) to haloperidol increases haloperidol levels, increasing QTc prolongation risk.
- Enzyme Induction: A drug increases CYP enzyme expression, accelerating metabolism. Example: Adding carbamazepine (CYP3A4 inducer) to aripiprazole reduces aripiprazole levels by up to 70%, potentially causing treatment failure.
4e. Genetic Polymorphisms
CYP2D6 is the most polymorphic psychiatric CYP enzyme. Phenotypes include:
- Poor Metabolizers (PM): 2 non-functional alleles. Standard doses cause toxic accumulation. ~7-10% of Caucasians, ~1-2% of Asians.
- Intermediate Metabolizers (IM): One reduced-function allele. Moderate increases in drug exposure.
- Extensive Metabolizers (EM): Normal function. Standard dosing applies.
- Ultrarapid Metabolizers (UM): Gene duplication. Drugs metabolized too quickly; standard doses may be subtherapeutic. ~2-5% of population.
Pharmacogenomic testing (e.g., GeneSight) can identify a patient’s CYP2D6 and CYP2C19 phenotype and guide prescribing decisions.
5. How to Structure Your Concept Map
The rubric awards 10 points for concept map design and visual creativity. Below is a recommended layout that earns full marks.
Recommended Layout Structure
- Central Hub: Label it ‘Agonist Spectrum’ or ‘Receptor Activity Spectrum.’
- Four Branches: One per position — Full Agonist, Partial Agonist, Antagonist, Inverse Agonist. Use distinct colors for each branch.
- Each Branch Contains: (a) Definition + intrinsic efficacy value, (b) Receptor mechanism, (c) Linked medications from the assignment list.
- P450 Module: A separate but connected section. Show the enzyme subtypes, their drug substrates from the list, and the ADME pharmacokinetic roles.
- Visual Aids: Use color coding, icons (receptor diagrams, enzyme icons), arrows indicating agonist vs. antagonist effects, and a legend.
Color Coding Suggestion
| Agonist Type | Suggested Color |
| Full Agonist | Green (#1A7A4A) |
| Partial Agonist | Blue (#2E5FA3) |
| Antagonist | Purple (#7B3FA0) |
| Inverse Agonist | Red (#C0392B) |
APA Format Reminders
- Title page: Running head, title, student name, institution, course, date.
- In-text citations within concept map nodes for each pharmacological claim.
- Reference list on a final page — minimum 3-5 peer-reviewed sources (published within 5 years recommended).
- Suggested sources: Stahl’s Essential Psychopharmacology (Stahl, 2021), FDA prescribing information, peer-reviewed journals (Journal of Clinical Psychiatry, CNS Drugs).
6. Quick-Reference Summary Table
Use this as a final check before submitting your concept map:
| Drug | Spectrum | Primary CYP | Key Receptor(s) | Mechanism Summary |
| Oxycodone | Full Agonist | CYP3A4, CYP2D6 | Mu-opioid (MOR) | Full MOR activation → analgesia, respiratory depression |
| Amphetamine | Full Agonist (indirect) | CYP2D6 | DAT, NET reversal | Forces monoamine release; floods synapse with DA/NE |
| Aripiprazole | Partial Agonist | CYP3A4, CYP2D6 | D2, D3, 5-HT1A (partial); 5-HT2A (antagonist) | Stabilizes dopaminergic tone via partial D2 agonism |
| Brexpiprazole | Partial Agonist | CYP3A4, CYP2D6 | D2, 5-HT1A (partial); 5-HT2A, alpha-1A (antagonist) | Lower intrinsic D2 activity than aripiprazole; serotonin modulation |
| Haloperidol | Antagonist | CYP2D6, CYP3A4, CYP1A2 | D2 (primary), D1, alpha-1, H1 | Competitive D2 blockade; reduces positive psychotic symptoms |
| Naloxone | Antagonist | Glucuronidation (UGT) | Mu, kappa, delta-opioid | Competitive opioid receptor block; reverses overdose rapidly |
| Risperidone | Antagonist | CYP2D6 (primary) | D2, 5-HT2A, alpha-1, H1 | D2 + 5-HT2A dual block; atypical antipsychotic profile |
| Pimavanserin | Inverse Agonist | CYP3A4 (primary) | 5-HT2A (primary), 5-HT2C | Suppresses constitutive 5-HT2A activity; no dopamine activity |

References
- Stahl, S. M. (2021). Stahl’s essential psychopharmacology: Neuroscientific basis and practical applications (5th ed.). Cambridge University Press.
- U.S. Food and Drug Administration. (2023). Rexulti (brexpiprazole) prescribing information. Otsuka America Pharmaceutical.
- U.S. Food and Drug Administration. (2022). Abilify (aripiprazole) prescribing information. Otsuka America Pharmaceutical.
- U.S. Food and Drug Administration. (2021). Nuplazid (pimavanserin) prescribing information. Acadia Pharmaceuticals.
- Preskorn, S. H. (2020). Clinically relevant pharmacology of the cytochrome P450 system. Journal of Psychiatric Practice, 26(3), 201–217. https://doi.org/10.1097/PRA.0000000000000473
- Richelson, E. (2010). Receptor pharmacology of antipsychotics in relation to clinical effects. Journal of Clinical Psychiatry, 61(Suppl. 2), 5–14.
Assignment: Psychopharmacology Scavenger Hunt Concept Map
As you continue to learn about psychopharmacology, you will find that medications used to treat mental health conditions are agonists across the spectrum. It will be important for you to recognize some of those medications and how they act on a variety of neurochemicals in different ways to treat the symptoms.
In this Assignment, you will “scavenger” the literature as you research the agonist spectrum and key neurotransmitters and pathways targeted in psychopharmacology. You will have the opportunity to apply your knowledge as you create a Concept Map exploring each of the agonist spectrum listed below. Support your answers with evidence-based, peer-reviewed scholarly literature. APA style format title page, citations, and references will apply.
Note: You will not set up your Assignment as a paragraph-formatted paper but, instead, as a creative, visually appealing Concept Map.
Resources
Be sure to review the Learning Resources before completing this activity.
Click the weekly resources link to access the resources.
To prepare for this Assignment:
- Review the Learning Resources assigned this week.
- Review the Concept Map resources.
- Explore the listed agonist spectrum and consider the action and receptor of each:
- Agonist
- Partial agonist
- Antagonist
- Inverse agonist
The Assignment
You will submit a concept map exploring the four agonists on the agonist spectrum (agonist, partial agonist, antagonist, and inverse agonist) in which you:
- Describe the different characteristics of the four agonists and how each mediates distinct biological activities. Include proposed mechanisms and the receptor it is targeting.
- Identify how the P450 enzyme system plays a role in the body’s absorption, distribution, and clearance of medication.
- Scavenge the literature after describing each agonist on the spectrum for research that is based on the medications in the table below.
- Apply the medications to the appropriate agonist on the agonist spectrum in your Concept Map.
| Medications |
| Oxycodone |
| Brexpiprazole |
| Haloperidol |
| Naloxone |
| Aripiprazole |
| Amphetamine |
| Risperidone |
| Pimavanserin |
By Day 7 of Week 2
Submit by Day 7 of Week 2.
submission information
Before submitting your final assignment, you can check your draft for authenticity. To check your draft, access the Turnitin Drafts from the Start Here area.
- To submit your completed assignment, save your Assignment as WK2Assgn_LastName_Firstinitial
- Then, click on Start Assignment near the top of the page.