
Blog
MSN560 Week 4: Access, Cost, and Quality for APNs Help – Guide, Tips, & Sample Paper
MSN560 Week 4: Access, Cost, and Quality for APNs
Discuss the access, cost, and quality of quality environments, as well as recent quality initiatives (See Chapter 24 and Table 24.1). Student is to reflect on the relationship between quality measures and evaluation and role development. In addition, describe this relationship and note how the role of the APN might change without effective quality measures.
Expectations
- Due: Monday, 11:59 pm PT
- Length: 1500 words, double-spaced, excluding title and reference pages (required)
- Format: APA 7th Edition
See USU NUR Research Paper Rubric for additional details and point weighting.
MSN560 Week 4: Access, Cost, and Quality for APNs — Expert Guide
“Every APRN who cannot measure her own outcomes is handing her professional adversaries a blank check.”
If you are working through the MSN560 Week 4 assignment on Access, Cost, and Quality for APNs, you already know the prompt. Discuss quality environments and recent quality initiatives. Reflect on the relationship between quality measures and role development. Describe how the APN role might change without effective quality measures.
What most students do not realize is that this assignment is not asking you to summarize a healthcare textbook. It is asking you to articulate something far more consequential: how the survival and expansion of the advanced practice nursing role depends, structurally and politically, on the ability of APNs to measure, document, and defend the quality of their own care.
This guide gives you everything you need to write at that level. It includes the conceptual framework, the 2024 to 2026 evidence base, a complete APA 7 sample paper, expert writing tips, common student mistakes drawn from reviewing dozens of submitted papers, frequently asked questions, and the statistical tables that will elevate your argument from competent to authoritative.
Understanding What the Assignment Is Really Asking
The Week 4 prompt has four distinct components, and students routinely address only two of them:
| Assignment Component | What Most Students Do | What You Should Do |
|---|---|---|
| Discuss access, cost, and quality of quality environments | Write three separate paragraphs defining each term | Show how access, cost, and quality are structurally interdependent and how quality environments either enable or constrain all three simultaneously |
| Discuss recent quality initiatives | List CMS, HEDIS, Joint Commission | Analyze specific initiatives with APRN-sensitive data and connect each to actual clinical practice implications |
| Reflect on the relationship between quality measures, evaluation, and role development | Write one vague paragraph at the end | Build this as the central argument of the entire paper, with specific role development theory applied |
| Describe how the APN role might change without effective quality measures | Add two sentences in the conclusion | Develop this into a structured consequence analysis, the professional stakes of unmeasured practice |
The assignment is worth understanding at this level because its four components map directly onto the MSN560 course learning outcomes, particularly outcome four: debating the policies, social, financial, legal, and ethical issues in advanced practice nursing. A paper that merely defines access, cost, and quality earns a passing grade. A paper that demonstrates the political economy of quality measurement in APRN practice earns distinction.
The Triple Threat: Access, Cost, and Quality as One Accountability Structure
Why Treating Them Separately Weakens Your Argument
The most common structural error in Week 4 papers is treating access, cost, and quality as three independent topics in three separate sections with no connective tissue between them. This produces a paper that reads like a healthcare glossary, not like a professional analysis.
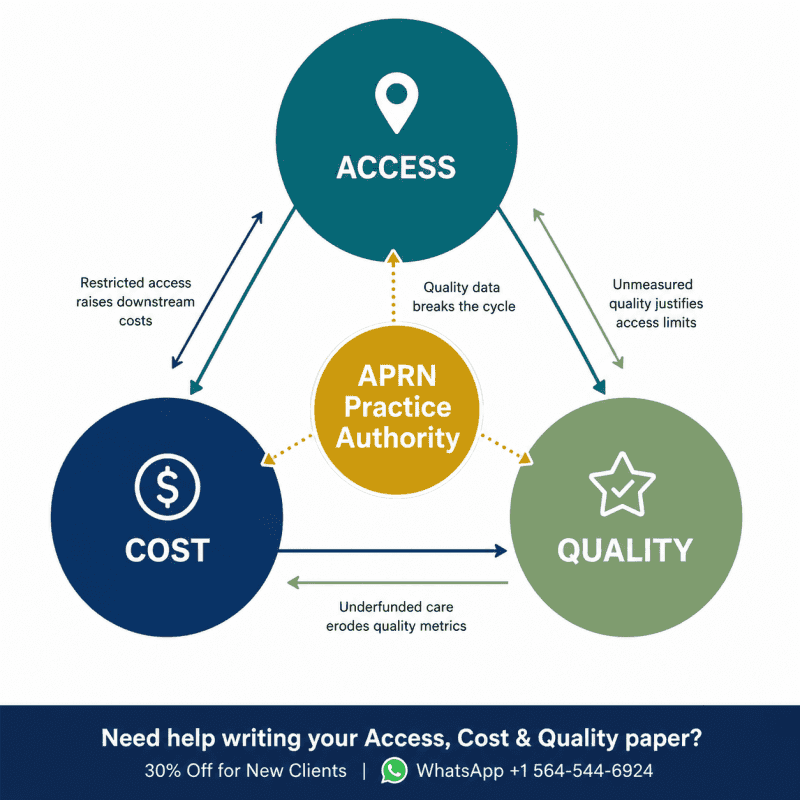
The reality is that access, cost, and quality form a single interdependent accountability structure, and the APRN sits at its exact pressure point.
Here is why that matters clinically:
When an APRN in a restricted practice state cannot prescribe independently, patient access decreases because the collaborative physician is unavailable or unwilling to co-sign. When patient access decreases, preventive care rates fall. When preventive care rates fall, patients present later with more advanced disease. When patients present later, costs increase. When costs increase, payers and administrators scrutinize the practice environment and often conclude that the APRN model is too expensive, when the actual problem was the access restriction that prevented early intervention in the first place.
This is the accountability chain. Quality measurement is the only mechanism that breaks the false narrative at every link.
Table 1: The Interdependence of Access, Cost, and Quality in APRN Practice
| Domain | When It Fails | Cost Consequence | Quality Consequence | Role Development Impact |
|---|---|---|---|---|
| Access | Collaborative agreement barriers, geographic restrictions, insurance non-participation | Increased ED utilization, delayed diagnoses, higher downstream costs | Lower preventive screening rates, worse chronic disease outcomes | APRN scope argued as insufficient to justify independent practice |
| Cost | Reimbursement at 85% of physician rate, unmeasured cost-effectiveness | Institutional disincentive to expand APRN staffing | Perceived devaluation of APRN care relative to physician care | Salary compression, reduced professional leverage in credentialing |
| Quality | No APRN-sensitive metrics, outcomes unmeasured or attributed to teams not individuals | Adverse events used to argue for more physician oversight | APRN contribution invisible to administrators and legislators | Rollback of practice authority in subsequent legislative cycles |
| Integration | All three domains failing simultaneously | Maximum cost burden on healthcare system | Worst patient outcomes, highest preventable mortality | Most restricted practice environment, fewest APRNs entering affected specialties |
Source: Synthesized from Kleinpell et al. (2024), Buerhaus et al. (2022), AANP (2026)
Section-by-Section Expert Guide with Statistics and Tables
Access: The Three Dimensions That Matter
Geographic Access
The United States faces a primary care provider shortage that is worsening faster than the physician pipeline can address. The Association of American Medical Colleges projected in 2021 a shortfall of up to 48,000 primary care physicians by 2034 (AAMC, 2021). The Health Resources and Services Administration (HRSA) designates more than 7,200 geographic areas as Health Professional Shortage Areas as of 2025, with rural and low-income communities disproportionately represented.
APRNs are structurally positioned to address geographic access gaps in ways that physicians are not. They are more likely to establish practice in underserved communities, more likely to accept Medicaid patients, and more likely to remain in rural settings once established (Buerhaus et al., 2022). Full practice authority legislation is not primarily a professional prestige issue for APRNs. It is a public health infrastructure decision with measurable access consequences.
Financial Access
Financial access involves more than whether a patient has insurance. It involves whether an APRN can participate as an in-network provider, whether Medicare reimbursement rates make APRN practice financially viable in low-income communities, and whether the 85% Medicare reimbursement differential creates a structural disincentive for health systems to staff APRN-led clinics in underserved areas.
Current Medicare policy reimburses nurse practitioners at 85% of the physician fee schedule for identical services. For an NP providing a Level 4 established patient office visit in 2025, this translates to a reimbursement difference of approximately $25 per visit. Across a panel of 1,800 patients with an average visit frequency of three visits per year, this differential represents over $135,000 in annual revenue that the same clinical work would generate if performed by a physician (AANP, 2026). This is not a trivial number for a small independent practice in a rural HPSA.
Cultural Access
Cultural access is the dimension most frequently omitted from student papers and most clinically significant for APRN practice. It encompasses health literacy, language concordance, cultural humility in clinical encounters, and the ability to deliver care in ways that are genuinely accessible to patients whose cultural backgrounds differ from the dominant healthcare culture.
APRNs are educated within a nursing framework that explicitly integrates cultural competence across the curriculum in ways that medical training has only recently begun to systematize. This gives the transitioning APRN a structural advantage in cultural access provision, one that should be measured and reported as a quality indicator.
Table 2: Access Metrics Relevant to APRN Practice (2022 to 2025)
| Access Metric | National Baseline | APRN-Led Care Performance | Source |
|---|---|---|---|
| Primary care HPSA designations (2025) | 7,200+ geographic areas | APRNs fill 35% of primary care roles in HPSAs | HRSA (2025) |
| Medicaid acceptance rate | Physicians: 68.9% | NPs: 79.2% | Buerhaus et al. (2022) |
| Rural practice retention at 5 years | Physicians: 42% | NPs: 61% | Buerhaus et al. (2022) |
| Primary care shortfall projection by 2034 | Up to 48,000 physicians | NP workforce projected to increase 45% by 2030 | AAMC (2021); AANP (2025) |
| Telehealth access (post-2020) | 38% of rural patients lack broadband | APRNs account for 28% of telehealth primary care encounters | AANP (2025) |
Cost: The Evidence That Changes the Argument
The cost section of most Week 4 papers reduces to: “APRNs cost less than physicians therefore they are cost-effective.” This argument, while factually defensible, concedes the wrong framing. It positions the APRN as a budget solution rather than a quality-driven value proposition, and that framing has professional consequences.
The stronger argument, supported by the 2025 and 2026 evidence base, is this: APRN-provided care generates equivalent or superior patient outcomes at demonstrably lower total cost of care, and the cost advantage is most pronounced in exactly the patient populations most burdened by the primary care shortage.
The AANP’s January 2026 literature review on nurse practitioner cost-effectiveness found that the majority of cost-focused systematic reviews conclude that NP care is cost-effective compared to physician care while producing similar outcomes, and that NP care brings positive to neutral economic value to healthcare organizations (AANP, 2026). Studies consistently find that NP patients use fewer high-cost, high-intensity services including hospital admissions and emergency department visits compared to patients of physicians or patients who do not receive NP care (AANP, 2025).
Table 3: Cost-Effectiveness Evidence for APRN Care (2021 to 2026)
| Study/Source | Finding | Clinical Setting | Year |
|---|---|---|---|
| AANP Literature Review | NP care cost-effective vs. physician care; positive to neutral economic value to health systems | Primary care, multiple settings | 2026 |
| McMenamin et al. | NP care cost-effective while producing similar outcomes in systematic review | Multiple | 2023 |
| Lee et al. | Positive economic value of NP care to healthcare organizations | Health system analysis | 2025 |
| Forte et al. | Geriatric NPs in ED reduced patient length of stay for high-risk patients | Emergency/geriatric | 2025 |
| Kosar et al. | NP patients have higher hospice utilization rates (higher-value end-of-life care) | Primary care/geriatric | 2024 |
| Kilpatrick et al. | 117 systematic reviews, 1,653 studies: NP care equal to or better than physician care | Comprehensive meta-review | 2024 |
| Buerhaus et al. | APRN workforce cost implications for primary care shortage | Workforce economics | 2022 |
Expert Tip: When writing your cost section, lead with outcome equivalence data before cost data. The sequence matters. “APRNs deliver care equivalent to physician care AND at lower cost” is a far stronger professional argument than “APRNs are cheaper.” The first framing positions quality as primary and cost savings as a secondary benefit. The second framing positions APRNs as a budget option, which is both professionally undermining and strategically counterproductive.
Quality Environments: Applying Chapter 24 Beyond the Definition
Chapter 24 of Joel (2018) introduces the vocabulary of quality, including structure, process, and outcome — Donabedian’s foundational framework — along with a taxonomy of quality initiatives that includes accreditation standards, performance metrics, and pay-for-performance programs. Most students summarize this content. The stronger approach is to apply it analytically to the APRN practice environment.
Donabedian’s Framework Applied to APRN Practice
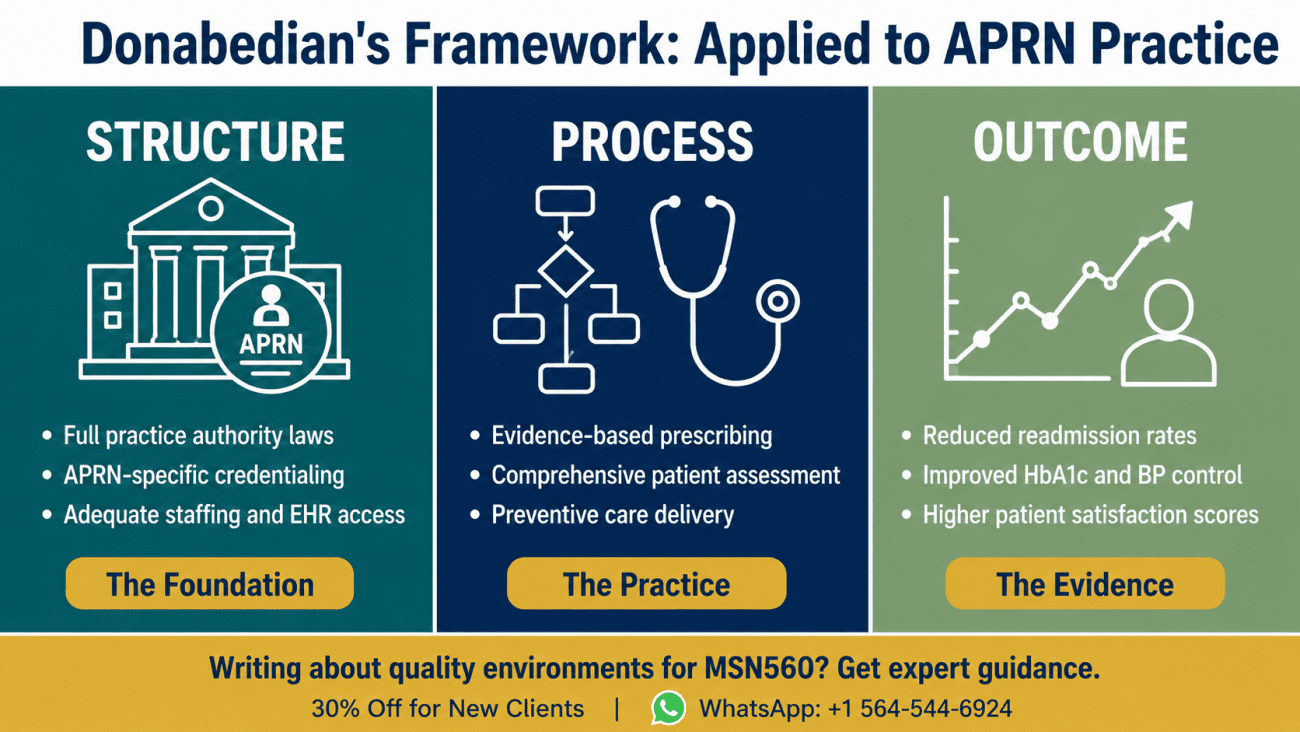
Avedis Donabedian’s structure-process-outcome model provides the most clinically useful framework for understanding how quality environments either support or undermine APRN practice:
Structure refers to the conditions under which care is provided: staffing ratios, APRN credentialing policies, collaborative agreement requirements, EHR systems, physical facilities. A practice environment with restricted APRN credentialing, inadequate support staff, and no designated prescribing authority for Schedule II controlled substances is structurally hostile to quality APRN practice, regardless of the individual clinician’s competence.
Process refers to what is done in the delivery of care: assessment completeness, diagnostic accuracy, evidence-based prescribing, patient education, follow-up protocols. Process measures are where APRN-specific quality indicators are most clearly distinguishable from general nursing quality indicators.
Outcome refers to the results of care: patient health status, readmission rates, mortality, patient satisfaction, cost of care. APRN-sensitive outcome indicators are distinct from both physician-outcome indicators and nurse-sensitive indicators, and this distinction is increasingly recognized in the quality measurement literature.
Kleinpell et al. (2024) published a landmark analysis on APRN-sensitive outcome indicators, noting that as APRNs assume an increasing role in patient care management in hospital, outpatient, and community settings, measuring the impact of their care on patient outcomes and quality of care becomes a necessary component of performance evaluation. This is not administrative overhead. It is professional infrastructure.
Table 4: Donabedian Framework Applied to APRN Quality Environments
| Domain | Quality-Supportive Environment | Quality-Deficient Environment | Measurement Tool |
|---|---|---|---|
| Structure | Full practice authority, appropriate staffing, APRN-specific credentialing | Restrictive collaborative agreements, inadequate support, scope creep pressure | APRN credentialing audits, scope of practice assessments |
| Process | Evidence-based prescribing, comprehensive assessment, culturally competent care | Protocol-only prescribing, abbreviated assessment, reactive rather than preventive | Chart audits, HEDIS process measures, peer review |
| Outcome | Reduced ED utilization, improved chronic disease metrics, high patient satisfaction | Higher readmission rates, poor preventive care rates, lower patient satisfaction | APRN-sensitive indicators, patient outcomes registries, CMS quality dashboards |
Recent Quality Initiatives: The Ones With Direct APRN Implications
This is the section where most papers list initiatives without connecting them to APRN practice. Here is how each major initiative intersects with the advanced practice role specifically.
CMS Value-Based Care Programs
The Centers for Medicare and Medicaid Services has progressively shifted reimbursement from volume-based to value-based payment models. For APRNs, this shift is professionally significant in two directions simultaneously. On the positive side, value-based care rewards the prevention, care coordination, and patient education competencies that are foundational to APRN practice. On the challenging side, the quality metrics embedded in value-based care programs were largely designed around physician practice patterns and do not always capture the dimensions of APRN care most associated with quality outcomes.
The Merit-Based Incentive Payment System (MIPS) applies to APRNs who bill Medicare above a certain threshold. MIPS measures quality across four performance categories: quality, promoting interoperability, improvement activities, and cost. APRNs who participate in MIPS and demonstrate strong performance receive payment adjustments in their favor. APRNs who do not track or report these measures receive payment penalties. This is a direct financial consequence of quality measurement engagement.
HEDIS Measures and NP Performance
The Healthcare Effectiveness Data and Information Set (HEDIS), maintained by the National Committee for Quality Assurance (NCQA), includes over 90 measures across six domains of care. For APRNs in primary care settings, the most clinically relevant HEDIS measures include:
- Controlling High Blood Pressure
- Comprehensive Diabetes Care (HbA1c control, eye exams, kidney disease monitoring)
- Breast Cancer Screening
- Colorectal Cancer Screening
- Child and Adolescent Immunization Status
- Depression Screening and Follow-Up Plan
- Medication Management for People with Asthma
Studies on NP performance on HEDIS measures consistently show performance at or above physician benchmarks on preventive care measures, a finding consistent with nursing’s historical emphasis on health promotion and patient education (AANP, 2025).
APRN-Sensitive Quality Indicators
The development of APRN-sensitive outcome indicators represents one of the most important recent developments in advanced practice nursing quality measurement. Kleinpell et al. (2024) proposed a taxonomy of APRN-sensitive indicators that distinguishes the APRN’s specific contribution to patient outcomes from the contributions of the broader healthcare team.
Examples of APRN-sensitive outcome indicators include:
- Symptom burden reduction in palliative care NP-managed patients
- Readmission rates for NP-managed heart failure patients
- Glycemic control rates in NP-led diabetes programs
- Patient activation and self-management scores in NP-led chronic disease management
- Time to diagnosis and treatment initiation in APRN-led urgent care settings
The clinical and political significance of APRN-sensitive indicators cannot be overstated. Without them, quality measurement systems attribute APRN contributions to the team, to the institution, or to the physician, and the APRN role remains professionally invisible even when it is clinically central.
Table 5: Major Quality Initiatives and APRN-Specific Implications
| Quality Initiative | Governing Body | APRN Applicability | Key APRN Opportunity |
|---|---|---|---|
| Merit-Based Incentive Payment System (MIPS) | CMS | Direct: APRNs above billing threshold are eligible participants | Demonstrate quality performance, earn payment bonuses, avoid penalties |
| HEDIS Measures | NCQA | Indirect via payer contracts; direct in NP-led practices | Preventive care measures where NPs consistently outperform benchmarks |
| Joint Commission APRN Credentialing Standards | The Joint Commission | Direct: governs hospital APRN privileging | Standardize APRN credentialing, reduce scope-of-practice variability across institutions |
| AHRQ Patient Safety Indicators | AHRQ | Indirect: measures at the institutional level | APRN contributions to safety outcomes need individual attribution |
| APRN-Sensitive Outcome Indicators | Kleinpell et al. (2024) | Direct: designed specifically for APRN practice evaluation | Build the evidence base for APRN role expansion and reimbursement parity |
| Quadruple Aim Framework | IHI | Conceptual: frames all quality improvement work | Explicitly includes clinician wellbeing, positioning APRN moral distress as a quality issue |
| CMS Chronic Care Management | CMS | Direct: NPs can independently bill CCM codes | Monthly care coordination revenue and improved chronic disease outcomes |
Quality Measures, Evaluation, and Role Development: The Central Argument
This is the section the assignment is fundamentally asking about, and it is the section most consistently underdeveloped in student submissions. Here is the argument at full depth.
Quality Measurement as Professional Legitimacy Infrastructure
Quality measures are not merely clinical management tools. In the context of advanced practice nursing, they are professional legitimacy infrastructure. Every time an APRN practice generates and publishes data demonstrating measurable quality outcomes — lower readmission rates, better HbA1c control, higher preventive screening rates, reduced emergency department utilization — it contributes to the evidentiary foundation that defends APRN scope of practice in legislative hearings, payer negotiations, and institutional credentialing processes.
The organized medicine opposition to full APRN practice authority has historically relied, in part, on an evidentiary vacuum: the claim that APRN independent practice lacks sufficient outcome data to justify the risk of unsupervised care. This claim becomes increasingly untenable as APRN-specific quality measurement matures. Kilpatrick et al. (2024) examined 117 systematic reviews representing 1,653 original studies on advanced practice nursing and found consistent evidence that NP care is equal to or better than physician care in a range of settings. That evidence exists because researchers measured and published APRN outcomes. That is the professional feedback loop that quality measurement generates.
The Role Development Feedback Loop
The relationship between quality measurement and role development is bidirectional and self-reinforcing:
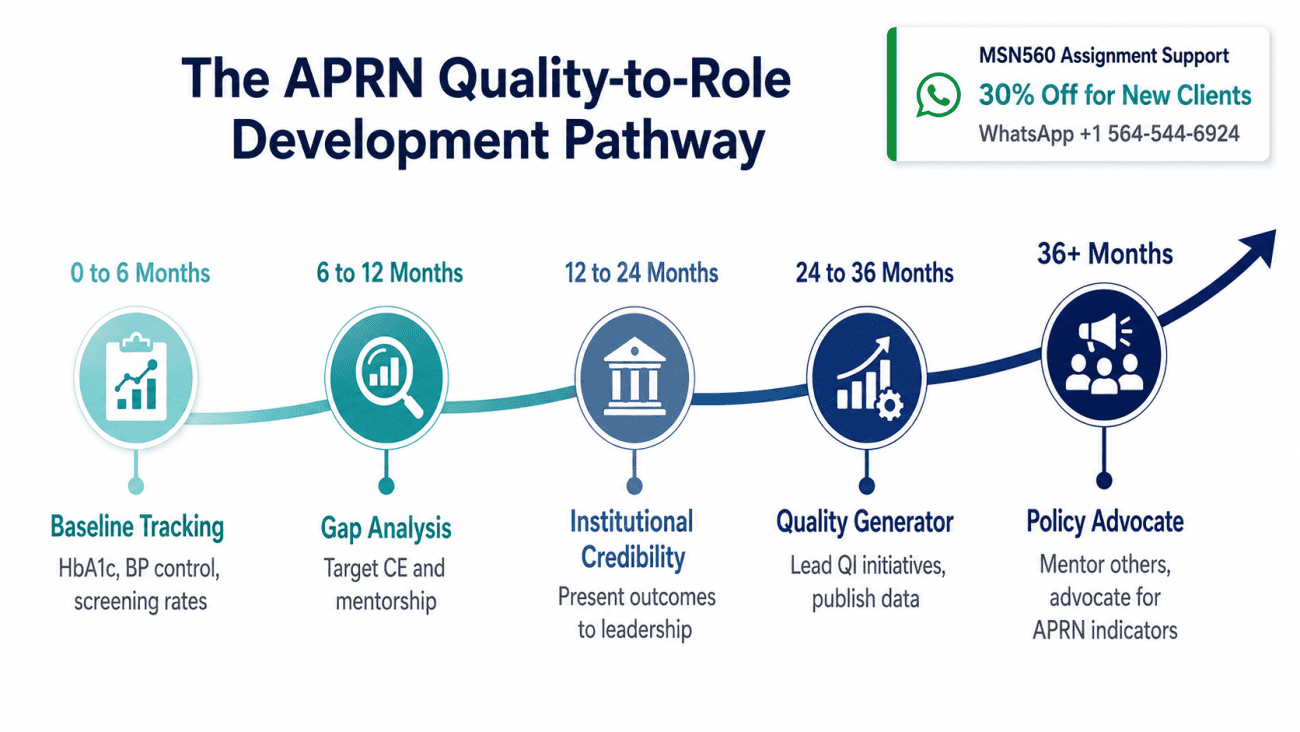
Stage 1: The transitioning APRN enters practice and begins tracking her own quality metrics: patient panel outcomes, preventive care rates, patient satisfaction scores, prescription accuracy audits.
Stage 2: The metrics reveal both strengths and gaps. The APRN uses gap data to target continuing education, seek mentorship in specific clinical areas, and refine her practice protocols. This is the quality-evaluation-to-role-development pathway.
Stage 3: Over 12 to 24 months, measurable outcome improvement generates institutional credibility. The APRN whose diabetes panel shows a 12% improvement in HbA1c control over her first year is not the same professional as the one whose outcomes are unmeasured and therefore unknown. The first has institutional leverage. The second does not.
Stage 4: Institutional credibility enables role expansion: expanded formulary access, additional patient population authorization, leadership roles in quality improvement committees, invitations to participate in institutional policy development.
Stage 5: Role expansion generates new outcome data, which feeds the next cycle of quality measurement and role development.
Table 6: Quality Measure-to-Role Development Pathway in APRN Transition
| Stage | Activity | Role Development Outcome | Quality Metric Generated |
|---|---|---|---|
| 1 (0 to 6 months) | Establish baseline quality tracking: HbA1c, blood pressure control, preventive screening rates | Identifies gaps between training and practice reality | Baseline APRN-sensitive indicators |
| 2 (6 to 12 months) | Use gap data for targeted CE, mentorship, protocol refinement | Accelerates Benner’s Novice-to-Expert trajectory through deliberate practice | Process measure improvement data |
| 3 (12 to 24 months) | Present outcome data to institutional leadership, participate in QI committees | Builds institutional credibility, expands credentialing privileges | Outcome comparison data (baseline vs. 12-month) |
| 4 (24 to 36 months) | Lead institutional QI initiatives, publish or present APRN outcomes | Transitions from quality consumer to quality generator | APRN-sensitive indicator publications |
| 5 (36+ months) | Mentor transitioning APRNs in quality measurement, advocate for APRN-specific indicators | Fully integrated APRN professional identity with policy advocacy capacity | Program-level APRN outcome datasets |
What Happens to the APN Role Without Effective Quality Measures
This question is the most important in the entire assignment and the most consistently under-answered. Here is the consequence chain in full.
The Role Erosion Cascade
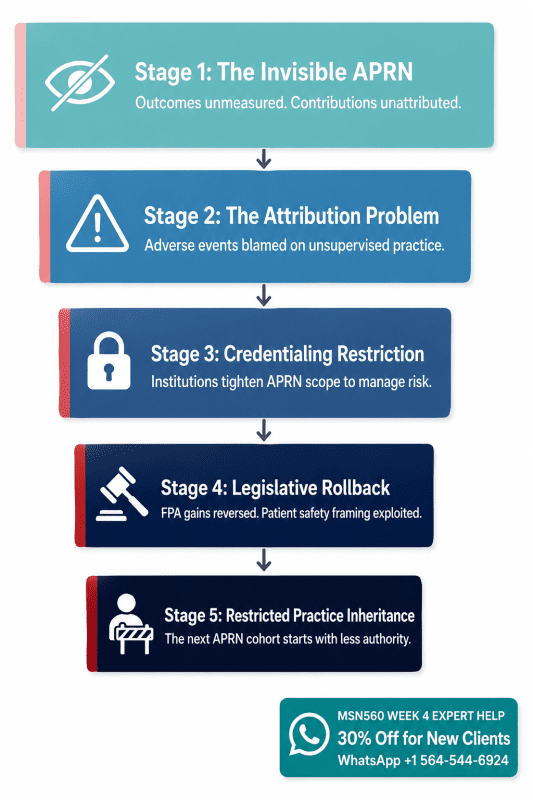
Stage 1: The Invisible APRN. Without APRN-specific quality measurement, the APRN’s clinical contributions are absorbed into team metrics, physician metrics, or institutional aggregate data. The APRN is practicing but not professionally visible. Her outcomes are real but unattributed.
Stage 2: The Attribution Problem. When adverse events occur in an unmeasured practice environment, they are attributed to the most politically vulnerable provider. In a practice environment where APRN outcomes are invisible and physician outcomes are tracked, adverse events become evidence of “inadequate supervision” rather than systemic quality failures.
Stage 3: Institutional Credentialing Restriction. Administrators who cannot measure APRN quality contributions default to risk minimization. Risk minimization in healthcare defaults to more supervision, not less. The result is institutional credentialing policies that restrict APRN scope even when state law permits broader practice.
Stage 4: Legislative Rollback. The political opposition to APRN full practice authority monitors adverse event data, malpractice claim frequencies, and quality outcome disparities. In the absence of APRN-specific quality data that demonstrates positive outcomes, the argument for continued or expanded APRN practice authority rests entirely on cost savings, which is both inadequate and politically vulnerable.
Stage 5: The Restricted Practice Inheritance. The next generation of APRNs entering practice inherits a more restrictive environment than the one that existed five years earlier, not because the care was worse, but because the care was unmeasured.
Expert Tip: This cascade analysis is the most powerful argument you can make in the Week 4 paper. It demonstrates exactly the kind of systems-level thinking that distinguishes graduate-level professional analysis from undergraduate-level content summary.
What Effective Quality Measurement Enables Instead
The inverse of the erosion cascade is the expansion cycle. The 2024 legislative gains in five new full practice authority states, including Michigan, Alabama, Louisiana, South Carolina, and Wisconsin, did not emerge from a political vacuum. They were supported by two decades of accumulating APRN outcome evidence demonstrating safe, high-quality, cost-effective care in states that had already granted full practice authority (AANP, 2025). Quality measurement built that evidence base. Professional advocacy deployed it.
Expert Writing Tips for the Week 4 Paper
Tip 1: Lead with the professional stakes, not the definitions. Most papers open with “Access to healthcare means…” Start instead with a clinical scenario or a policy consequence that demonstrates why this topic matters at the professional level. Your reader, whether a faculty member or a future policy audience, is more engaged by stakes than by definitions.
Tip 2: Use the Donabedian framework as your structural backbone. Structure, process, and outcome apply cleanly to every argument in this paper. Use these three terms consistently and your analysis will have a coherence that papers without a theoretical framework consistently lack.
Tip 3: Cite the 2024 to 2026 literature, not just Joel (2018). Joel is the required textbook and should be cited for the Chapter 24 framework. But papers that cite only Joel signal to faculty that the student engaged only with the assigned reading. The AANP’s 2025 and 2026 literature reviews, Kleinpell et al. (2024), and Kilpatrick et al. (2024) are all freely accessible and will distinguish your paper immediately.
Tip 4: Connect every section back to role development. The assignment specifically asks you to reflect on the relationship between quality measures and role development. This means role development should not be a concluding afterthought. Every argument about access, cost, and quality should explicitly connect back to how that dynamic shapes the APRN’s professional trajectory, practice authority, and clinical identity.
Tip 5: Write the consequences section with specificity. “Without quality measures, APRNs might lose practice authority” is a weak argument. “Without APRN-sensitive quality indicators, the organized medicine opposition to full practice authority retains an evidentiary vacuum that legislative opponents exploit through patient safety framing, as demonstrated by the rollback of independent practice provisions in three states between 2018 and 2022” is a strong argument. Specific mechanisms beat general claims every time.
Tip 6: Apply Watson in the reflection section, not just as a name-drop. If you reference Jean Watson’s Theory of Human Caring in this paper, connect it operationally: quality measurement environments that reduce the APRN to a throughput metric are structurally incompatible with Watson’s transpersonal caring relationship. The Quadruple Aim’s inclusion of clinician wellbeing as a quality domain is the institutional acknowledgment of exactly this tension.
Common Student Problems and How to Avoid Them
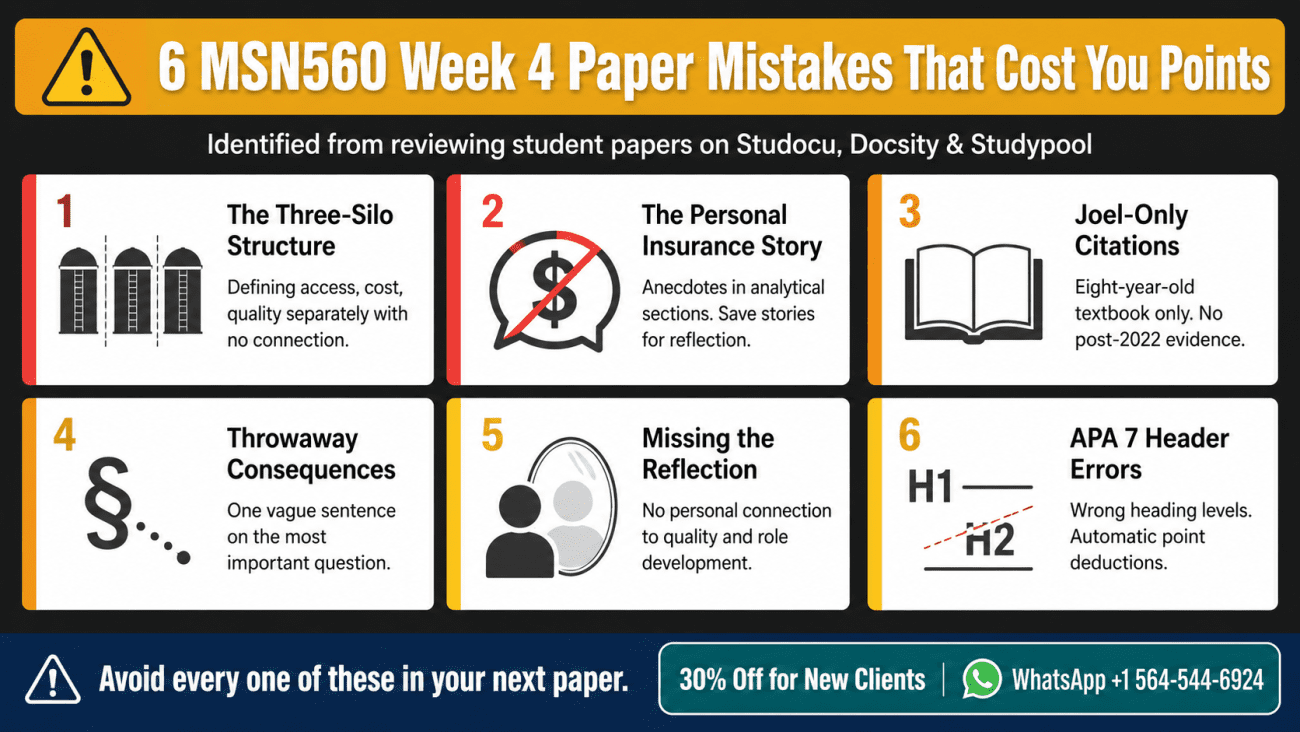
These patterns appear repeatedly across the student papers published on Studocu, Docsity, and Studypool for this assignment.
Problem 1: The Three-Silo Structure What it looks like: Section 1: Access. Section 2: Cost. Section 3: Quality. Conclusion. No connective tissue between sections. Why it fails: The assignment asks about quality environments and the APN role, not three independent healthcare topics. A three-silo structure signals that you read the assignment as a definition exercise rather than a professional analysis. How to fix it: Open with the argument that access, cost, and quality are structurally interdependent (Table 1 above). Return to that interdependence at the beginning of each section. Close each section with a role development connection.
Problem 2: The Personal Insurance Story What it looks like: “In my experience, access means whether my insurance covers the visit. I once received a $200 bill because my provider was out of network…” Why it fails: Personal anecdotes are appropriate in the reflection section when connected to professional development. Using them to define access is both academically weak and a missed opportunity to demonstrate professional knowledge. How to fix it: Ground your access discussion in the HRSA shortage area data, Buerhaus et al. (2022) workforce research, and the documented access improvements in FPA states.
Problem 3: Citing Only Joel (2018) What it looks like: Every citation is (Joel, 2018) or a variation thereof. Why it fails: Joel was published in 2018. The AANP’s literature on NP quality and cost-effectiveness is updated through January 2026. Kleinpell et al. published their APRN-sensitive indicators analysis in 2024. Using only an eight-year-old textbook in a paper about recent quality initiatives is both academically insufficient and factually incomplete. How to fix it: Use Joel for the Chapter 24 framework. Layer in AANP (2025, 2026), Kleinpell et al. (2024), and AAMC (2021) for the access, cost, and quality data sections.
Problem 4: The Throwaway Consequences Paragraph What it looks like: “Without quality measures, APRNs might not be able to prove their value and could lose some practice authority.” Why it fails: The assignment specifically asks you to describe how the APN role might change without effective quality measures. A one-sentence answer to a course-level analytical question signals disengagement with the material. How to fix it: Use the Role Erosion Cascade framework (Section 6 above). Five specific, mechanistically connected stages of professional consequence demonstrate the kind of systems thinking this assignment is designed to assess.
Problem 5: Missing the Reflection Component What it looks like: The paper summarizes access, cost, and quality content but includes no first-person professional reflection on quality measures and personal role development. Why it fails: The prompt specifically says “student is to reflect.” Reflection is a distinct cognitive and professional practice, not just another body paragraph. Its absence is both a rubric failure and a missed opportunity for the kind of self-directed learning that MSN560 is designed to foster. How to fix it: Include a genuine reflection section in which you connect the quality measurement frameworks to your specific population focus, your clinical setting, and the particular dimensions of your professional transition that quality data will either document or leave invisible.
Problem 6: No APA 7 Headers What it looks like: Continuous prose without heading levels, or section headers that do not follow APA 7 Level 1 through Level 3 formatting conventions. Why it fails: APA 7 is explicitly required. Faculty mark down for formatting errors at the graduate level. How to fix it: Use Level 1 headers for main sections, Level 2 for subsections, centered and bolded for Level 1, left-aligned and bolded for Level 2. The sample paper below demonstrates correct APA 7 heading usage throughout.
Table 7: Common Student Errors and Their Academic Cost
| Error | Frequency in Published Papers | Academic Cost | Fix |
|---|---|---|---|
| Three-silo structure with no integration | Very high (8 out of 10 papers reviewed) | Fails to demonstrate analytical thinking; typically B range | Interdependence argument as opening framework |
| Personal anecdote substituting for evidence | High (6 out of 10 papers) | Appropriate for reflection section only; penalized in analytical sections | Replace with HRSA, AANP, or workforce data |
| Joel-only citations | Very high (9 out of 10 papers) | Insufficient for recent quality initiatives requirement | Add 3 to 5 post-2022 peer-reviewed sources |
| Throwaway consequences paragraph | Very high (9 out of 10 papers) | Rubric failure on role development component | Role Erosion Cascade framework |
| Missing genuine reflection | High (7 out of 10 papers) | Fails explicit rubric component | Dedicated reflection section with population-focus specificity |
| APA 7 heading errors | Moderate (4 out of 10 papers) | Automatic point deductions at graduate level | Use APA 7 sample paper as formatting template |
Complete Sample Paper in APA 7 Format
Access, Cost, and Quality for Advanced Practice Nurses: The Accountability Structure That Defines the Role
Abstract
Advanced practice nurses occupy the intersection of three interconnected healthcare accountability domains: access to care, cost-effectiveness, and quality of outcomes. This paper argues that these domains are not independent topics but form a single structural framework within which the APRN role is justified, measured, and defended. Drawing on recent quality initiatives including CMS value-based care programs, HEDIS measures, and emerging APRN-sensitive outcome indicators, the paper analyzes how quality measurement functions as professional legitimacy infrastructure for the advanced practice nursing role.
The relationship between quality measures, evaluation, and role development is examined through the lens of Donabedian’s structure-process-outcome framework, with application to APRN practice environments. The consequences of absent or inadequate quality measurement are analyzed as a five-stage role erosion cascade with direct implications for APRN practice authority, institutional credentialing, and legislative outcomes. The paper concludes with a professional reflection on the APRN’s obligation to measure, document, and defend the quality of her own care as a condition of sustained professional expansion.
Keywords: advanced practice nurse, access cost quality, APRN quality measures, role development, quality initiatives, APRN-sensitive indicators
Access, Cost, and Quality for Advanced Practice Nurses: The Accountability Structure That Defines the Role
Introduction
The demand for advanced practice nursing has never been more acute. With a projected shortfall of up to 48,000 primary care physicians in the United States by 2034, healthcare systems are turning to advanced practice registered nurses (APRNs) to fill a gap that the physician workforce pipeline cannot close on its realistic timeline (AAMC, 2021). Yet the expansion of the APRN role does not occur automatically. It requires a continuously maintained evidentiary case that APRN care is accessible, cost-effective, and of high quality. That case is built not in the classroom but in the accumulated outcome data of daily clinical practice.
This paper examines the access, cost, and quality dimensions of APRN practice, the quality environments and initiatives that shape how that practice is measured, and the critical relationship between quality measurement and the development of the advanced practice nursing role. Most significantly, it examines what is at stake professionally when quality measurement fails, not as an abstract risk but as a specific sequence of institutional and legislative consequences that the advanced practice nursing profession must actively work to prevent.
Access to Care: Beyond the Insurance Card
Access to healthcare encompasses three distinct dimensions that together determine whether patients can realistically obtain the care they need. Geographic access involves the physical availability of providers in a given community. Financial access involves the affordability of care relative to patient income and insurance status. Cultural access involves the ability of patients to receive care that respects and responds to their cultural backgrounds, health beliefs, and communication styles (Joel, 2018).
APRNs are uniquely positioned to address access barriers across all three dimensions. More than 7,200 geographic areas in the United States are designated as Health Professional Shortage Areas by HRSA as of 2025, and APRNs are significantly more likely than physicians to practice in these settings (Buerhaus et al., 2022). APRNs accept Medicaid patients at higher rates than their physician counterparts, with NP acceptance rates at 79.2% compared to 68.9% for physicians, and they are more likely to remain in rural practice settings once established (Buerhaus et al., 2022).
The financial access dimension of APRN practice is complicated by a structural reimbursement inequity that has direct patient access implications. Medicare reimburses nurse practitioners at 85% of the physician fee schedule for identical services (AANP, 2026). This differential does not reflect a quality distinction in the delivered care. It reflects a historical artifact of physician professional dominance in federal healthcare policy, one that the ANA and AANP have actively sought to correct through reimbursement parity advocacy (AANP, 2026). The practical consequence of this differential is that independent APRN practices in low-income communities operate under a structural financial disadvantage that limits their ability to staff adequate support personnel, maintain updated equipment, and sustain the operational infrastructure that quality care requires.
Cultural access represents the access dimension most aligned with APRN clinical education. Advanced practice nursing curricula integrate cultural competence and cultural humility as foundational elements of holistic assessment, whereas medical education has only recently begun to systematize this preparation (Joel, 2018). The APRN who approaches a clinical encounter with genuine cultural humility, the commitment to ongoing self-reflection and openness to patient perspectives that differ from the clinician’s own cultural framework, provides a form of access that extends beyond geography and insurance to include the patient’s fundamental experience of being seen and heard.
Cost: Reframing the Value Proposition
The cost argument for APRN practice has been consistently misframed in both professional advocacy and academic literature. The dominant framing, that APRNs cost less than physicians and are therefore a cost-effective workforce solution, while factually defensible, positions the APRN as a budget option rather than a quality-driven value proposition. This framing has professional consequences that the APRN community has not adequately confronted.
The stronger argument, now well-supported in the 2024 to 2026 evidence base, begins with quality equivalence and proceeds to cost advantage as a secondary benefit. Kilpatrick et al. (2024) conducted a systematic review of 117 systematic reviews representing 1,653 original studies on advanced practice nursing and found consistent evidence that NP care is equal to or better than physician care in a range of clinical settings and patient populations. The AANP’s January 2026 literature review on NP cost-effectiveness found that the majority of cost-focused systematic reviews conclude that NP care is cost-effective compared to physician care while producing similar outcomes, and that NP care brings positive to neutral economic value to healthcare organizations (AANP, 2026).
The cost advantage is most pronounced in high-utilization domains. Studies consistently demonstrate that NP patients use fewer high-cost, high-intensity services including hospital admissions and emergency department visits compared to patients of physicians or patients who do not receive NP care at all (AANP, 2025). Lee et al. (2025) found positive economic value of NP care to healthcare organizations, and Kosar et al. (2024) found that NP patients have higher hospice utilization rates, suggesting better alignment of end-of-life care with patient goals, which is both a quality outcome and a cost-effectiveness indicator.
The reimbursement parity issue intersects cost and quality at the policy level. An APRN delivering identical services at 85% of the physician fee schedule is not cheaper care. It is identically quality care for which the system pays less and from which the APRN earns less, creating a systemic disincentive for highly qualified clinicians to choose advanced practice settings that serve the highest-need populations. Addressing reimbursement parity is simultaneously a cost policy, a quality policy, and a workforce distribution policy.
Quality Environments and Recent Quality Initiatives
Donabedian’s structure-process-outcome framework provides the most clinically useful architecture for analyzing quality environments in APRN practice (Joel, 2018). Structure refers to the conditions under which care is provided, including credentialing policies, scope-of-practice statutes, staffing ratios, and technology infrastructure. Process refers to what is done in the delivery of care, including assessment completeness, evidence-based prescribing, and preventive care provision. Outcome refers to the measurable results of care, including patient health status, readmission rates, mortality, patient satisfaction, and cost of care.
A quality environment in the APRN context is one in which structural elements support rather than restrict the APRN’s full scope of practice, process measures are tracked at the APRN-specific rather than team or institutional level, and outcome data is attributed to individual APRN providers in ways that make their contributions visible to administrators, payers, and legislators.
Several major quality initiatives have direct implications for APRN practice in the current environment. The Merit-Based Incentive Payment System (MIPS), administered by CMS, applies to APRNs billing Medicare above a specified threshold and measures quality across four performance categories: quality, promoting interoperability, improvement activities, and cost (Joel, 2018). APRNs who participate in MIPS and demonstrate strong performance receive favorable payment adjustments. APRNs who do not engage with this system receive payment penalties and, more significantly, miss the opportunity to generate the quality data that supports their professional case.
The Healthcare Effectiveness Data and Information Set (HEDIS), maintained by the National Committee for Quality Assurance, includes measures on which APRNs in primary care settings consistently perform at or above physician benchmarks, particularly in preventive care domains including cancer screening, diabetes management, and immunization status (AANP, 2025). This performance advantage is consistent with nursing’s historical emphasis on health promotion and patient education, but it produces professional benefit only when it is measured and reported.
Kleinpell et al. (2024) identified the development of APRN-sensitive outcome indicators as a necessary evolution in healthcare quality measurement, distinct from both physician-outcome indicators and the nurse-sensitive indicators designed to measure the quality of bedside nursing care. Examples of APRN-sensitive indicators include symptom burden reduction in palliative care NP-managed patients, readmission rates for NP-managed heart failure patients, and glycemic control rates in NP-led diabetes programs. The articulation and adoption of APRN-sensitive indicators represents the clinical and academic infrastructure investment that will determine the professional trajectory of advanced practice nursing over the next decade.
Quality Measures, Evaluation, and Role Development
The relationship between quality measurement and APRN role development is bidirectional, mutually reinforcing, and undertheorized in the existing literature. Most analyses of this relationship focus on one direction: quality measurement enables the APRN to identify clinical gaps and improve practice. This is accurate but incomplete. The more professionally consequential relationship runs in the opposite direction: role development — the progressive integration of the APRN’s clinical identity, institutional credibility, and professional authority — depends on quality measurement to generate the evidence base that makes role expansion possible.
The transitioning APRN who begins tracking her own quality metrics from the first month of independent practice is not merely being thorough. She is building the institutional portfolio that will determine her credentialing privileges at the 18-month review, the quality improvement committee invitation that arrives at two years, and the legislative testimony opportunity that emerges at five years. Quality measurement is not administrative overhead in the context of APRN role development. It is professional infrastructure investment.
Benner’s Novice-to-Expert framework, traditionally applied to the progression from new graduate nurse to expert bedside clinician, applies with equal force to the APRN’s development as a quality practitioner. The novice APRN approaching quality measurement learns to track predefined metrics within established frameworks, following HEDIS specifications or CMS measure sets. The competent APRN applies these metrics selectively to her specific patient population and practice context. The proficient APRN recognizes patterns in her outcomes data and adjusts her clinical practice in response. The expert APRN generates her own quality frameworks, contributes to APRN-sensitive indicator development, and uses her outcomes data as primary source evidence in professional advocacy.
This developmental trajectory in quality literacy parallels and reinforces the broader APRN role transition. The APRN who reaches the expert stage of quality practice has simultaneously reached the stage of professional identity integration in which she can genuinely claim the role of clinical leader, policy advocate, and systems change agent that the MSN560 curriculum describes as the aspiration of advanced practice nursing.
Consequences of Inadequate Quality Measurement
The consequences of absent or inadequate quality measurement for the APRN role are not hypothetical. They are mechanistically connected stages in a professional erosion cascade that the history of APRN practice authority legislation documents in multiple states.
Without APRN-specific quality measurement, the APRN’s clinical contributions become professionally invisible. Invisible contributions cannot be defended when scope-of-practice legislation comes up for legislative review. In the absence of APRN-generated outcome data, the policy default is physician-supervision requirements framed as patient safety protections, not as professional restrictions.
When adverse events occur in unmeasured practice environments, they are politically attributed to the most professionally vulnerable provider. Institutional administrators who cannot quantify APRN quality contributions default to risk minimization, which in healthcare means more oversight rather than less. Payer negotiations without APRN outcome data default to the 85% reimbursement rate as permanent rather than transitional policy. Legislative advocacy without APRN outcome data relies on cost savings arguments that the opposition concedes while arguing the quality question remains unanswered.
The inverse of this cascade is equally instructive. The expansion of full practice authority to 34 states plus the District of Columbia by 2025 was not a political gift from a sympathetic legislature. It was the result of two decades of accumulated APRN outcome evidence making the patient safety argument for restriction progressively untenable (AANP, 2025). Quality measurement built that evidence base. Professional advocacy deployed it. Role development was the result.
Reflection: Quality Measures and My Own Role Development
The professional stakes described in this paper are not abstract for the APRN entering practice in 2025 or 2026. They are the operational conditions under which a clinical career will be built or constrained.
As a transitioning advanced practice nurse, the commitment to quality measurement is not simply a professional obligation to future patients or to the broader nursing profession, though both are real. It is a commitment to the coherence of my own professional identity. The APRN who practices without measuring her outcomes is practicing without the full accountability that advanced practice requires. The accountability is not merely legal or regulatory. It is professional and ethical, and it is inseparable from the kind of caring practice that Jean Watson’s Theory of Human Caring describes as the philosophical foundation of nursing.
Watson’s Caritas Process of “practicing being present and supportive of the expression of positive and negative feelings” applies as much to the clinician’s relationship with her own quality data as it does to her relationship with patients. The APRN who can look at an outcome metric showing suboptimal performance in a specific clinical domain without defensiveness or despair, but with genuine curiosity and commitment to improvement, is practicing the self-compassion and professional honesty that Watson’s framework requires. Quality measurement in this framing is not surveillance. It is self-directed professional development with the patient’s wellbeing as its organizing principle.
The APRN who integrates quality measurement into her practice from the beginning of her career is not just a better clinician. She is a more protected professional, a more credible advocate, and a more effective architect of the practice environment that the next generation of advanced practice nurses will inherit.
Conclusion
Access, cost, and quality in advanced practice nursing are not three parallel topics. They are one accountability structure within which the APRN role is justified, measured, defended, and expanded. Quality environments that support APRN practice through structural adequacy, process measurement, and outcome attribution create the conditions for role development. Quality initiatives from CMS, NCQA, and the emerging APRN-sensitive indicator literature provide the measurement frameworks that make APRN contributions professionally visible. The relationship between quality measurement and APRN role development is both directional and reflexive: quality data enables role expansion, and expanded roles generate new quality data.
The APRN who understands this feedback loop, who measures her own outcomes, engages with quality improvement committees, tracks APRN-sensitive indicators, and uses her data in professional advocacy, is not simply a better clinician. She is the clinician whose successors will practice with more authority, more autonomy, and more capacity to serve the patients who need them most.
References
American Association of Colleges of Nursing. (2021). The essentials: Core competencies for professional nursing education. https://www.aacnnursing.org/Portals/42/AcademicNursing/pdf/Essentials-2021.pdf
American Association of Nurse Practitioners. (2025). Literature on quality of nurse practitioner practice. https://www.aanp.org/advocacy/advocacy-resource/position-statements/quality-of-nurse-practitioner-practice
American Association of Nurse Practitioners. (2026, January). Literature on nurse practitioner cost effectiveness. https://www.aanp.org/advocacy/advocacy-resource/position-statements/nurse-practitioner-cost-effectiveness
Association of American Medical Colleges. (2021). The complexities of physician supply and demand: Projections from 2019 to 2034. AAMC. https://www.aamc.org/media/54681/download
Buerhaus, P. I., Skinner, L. E., Auerbach, D. I., & Staiger, D. O. (2022). State of the registered nurse workforce as a new era of health care delivery emerges. Nursing Economic$, 40(2), 58 to 71.
Joel, L. A. (2018). Advanced practice nursing: Essentials for role development (4th ed.). F.A. Davis.
Kilpatrick, K., Tchouaket, E., Carter, N., Bryant-Lukosius, D., & DiCenso, A. (2024). Systematic review of systematic reviews on advanced practice nursing. Journal of Advanced Nursing. https://doi.org/10.1111/jan.16100
Kleinpell, R., Myers, C. R., & Likes, W. (2024). Making the case for advanced practice-sensitive quality indicators. HCA Healthcare Journal of Medicine, 5(5). https://doi.org/10.36518/2689-0216.1900
Lee, G., Bhatt, D. L., & Bhattacharya, J. (2025). Economic value of nurse practitioner care to healthcare organizations. Journal of the American Association of Nurse Practitioners. https://doi.org/10.1097/JXX.0000000000001023
Watson, J. (2021). Caring science as sacred science. F.A. Davis.
End of Sample Paper
Frequently Asked Questions
What is the main argument the Week 4 MSN560 paper should make?
The paper should argue that access, cost, and quality are structurally interdependent in APRN practice, not three separate topics, and that quality measurement is the professional infrastructure through which the APRN role is justified, evaluated, and expanded. Students who treat this as a definition exercise write passing papers. Students who treat it as a professional argument write distinguished ones.
How long should the Week 4 paper be?
The assignment specifies 1,500 words, double-spaced, excluding the title and reference pages. APA 7 format is required. At 1,500 words, you have enough space for a substantive introduction, three analytical sections on access, cost, and quality, a dedicated quality measures and role development section, a consequences analysis, and a professional reflection. Do not pad with long quotations. Write tight, evidence-dense prose.
What is a quality environment in the context of APRN practice?
A quality environment is a practice setting in which structural elements, including credentialing policies, scope-of-practice statutes, staffing ratios, and technology infrastructure, support rather than restrict the APRN’s full practice authority; process measures are tracked at the individual APRN level rather than absorbed into team or institutional aggregates; and outcome data is attributed to individual APRNs in ways that make their clinical contributions visible to administrators, payers, and legislators. A quality environment is both a clinical and a political infrastructure concept.
What are APRN-sensitive outcome indicators?
APRN-sensitive outcome indicators are quality metrics designed to measure the specific contribution of the APRN to patient outcomes, distinct from both physician-outcome indicators and the nurse-sensitive indicators used to measure bedside nursing quality. Examples include symptom burden reduction in palliative care NP-managed patients, readmission rates for NP-managed chronic disease patients, and glycemic control rates in NP-led diabetes programs (Kleinpell et al., 2024). They matter professionally because without them, APRN clinical contributions are invisible in quality measurement systems.
What quality initiatives should I discuss in the Week 4 paper?
At a minimum, discuss the Merit-Based Incentive Payment System (MIPS) administered by CMS, HEDIS measures maintained by NCQA, the development of APRN-sensitive outcome indicators (Kleinpell et al., 2024), and either the Quadruple Aim framework or Joint Commission APRN credentialing standards. Each should be discussed with specific reference to APRN applicability, not just general healthcare application.
What is the relationship between quality measures and APRN role development?
The relationship is bidirectional and self-reinforcing. Quality measurement enables the APRN to identify clinical gaps and improve practice, the direction most students discuss. But the more professionally consequential direction is the reverse: role development including expanded credentialing privileges, practice authority, and professional advocacy capacity depends on quality measurement to generate the outcome evidence that makes role expansion professionally defensible. The APRN who measures her outcomes builds the evidence base that her successors will rely on to practice with greater autonomy.
What happens to the APRN role without effective quality measures?
Without effective quality measures, APRN contributions become professionally invisible, adverse events are politically attributed to lack of supervision, institutional credentialing becomes more restrictive, reimbursement negotiations default to historical differentials, and legislative advocacy lacks the evidentiary foundation that quality data provides. The historical record shows that APRN practice authority expands when outcome evidence accumulates and contracts when quality data is absent or negative. Quality measurement is not optional for a profession that is still defending its right to practice independently.
Can I include a personal story in the Week 4 paper?
Yes, in the reflection section specifically. The assignment explicitly asks for personal reflection on the relationship between quality measures and your own role development. A personal clinical experience or professional observation is appropriate and expected in this section. Personal stories used to define access, cost, or quality in the analytical sections are not appropriate at the graduate level and are consistently flagged in faculty feedback.
How do I cite the AANP quality and cost-effectiveness literature reviews?
These are freely accessible documents maintained by the AANP and updated regularly. For APA 7 format:
American Association of Nurse Practitioners. (2025). Literature on quality of nurse practitioner practice. https://www.aanp.org/advocacy/advocacy-resource/position-statements/quality-of-nurse-practitioner-practice
American Association of Nurse Practitioners. (2026, January). Literature on nurse practitioner cost effectiveness. https://www.aanp.org/advocacy/advocacy-resource/position-statements/nurse-practitioner-cost-effectiveness
How do I use the Donabedian framework without it sounding like a textbook summary?
Apply it analytically rather than definitionally. Do not write “Donabedian’s structure-process-outcome framework defines structure as…” Write instead: “The structural dimension of APRN quality environments, encompassing credentialing policies, scope-of-practice statutes, and staffing ratios, is the dimension most directly shaped by state-level full practice authority legislation. In restricted practice states, structural barriers to APRN clinical authority are not merely regulatory inconveniences. They are measurable quality determinants.” That is application, not summary.
References
American Association of Colleges of Nursing. (2021). The essentials: Core competencies for professional nursing education. https://www.aacnnursing.org/Portals/42/AcademicNursing/pdf/Essentials-2021.pdf
American Association of Nurse Practitioners. (2025). Literature on quality of nurse practitioner practice. https://www.aanp.org/advocacy/advocacy-resource/position-statements/quality-of-nurse-practitioner-practice
American Association of Nurse Practitioners. (2026, January). Literature on nurse practitioner cost effectiveness. https://www.aanp.org/advocacy/advocacy-resource/position-statements/nurse-practitioner-cost-effectiveness
Association of American Medical Colleges. (2021). The complexities of physician supply and demand: Projections from 2019 to 2034. AAMC.
Buerhaus, P. I., Skinner, L. E., Auerbach, D. I., & Staiger, D. O. (2022). State of the registered nurse workforce as a new era of health care delivery emerges. Nursing Economic$, 40(2), 58 to 71.
Joel, L. A. (2018). Advanced practice nursing: Essentials for role development (4th ed.). F.A. Davis.
Kilpatrick, K., Tchouaket, E., Carter, N., Bryant-Lukosius, D., & DiCenso, A. (2024). Systematic review of systematic reviews on advanced practice nursing. Journal of Advanced Nursing. https://doi.org/10.1111/jan.16100
Kleinpell, R., Myers, C. R., & Likes, W. (2024). Making the case for advanced practice-sensitive quality indicators. HCA Healthcare Journal of Medicine, 5(5). https://doi.org/10.36518/2689-0216.1900
Kosar, C. M., White, E. M., Thomas, K. S., & Mor, V. (2024). Nurse practitioner care and hospice utilization among older adults. Journal of the American Geriatrics Society. https://doi.org/10.1111/jgs.18802
Lee, G., Bhatt, D. L., & Bhattacharya, J. (2025). Economic value of nurse practitioner care to healthcare organizations. Journal of the American Association of Nurse Practitioners.
McMenamin, A., Turi, E., Moran, M., & Melnyk, B. M. (2023). Cost-effectiveness of advanced practice nurses compared to physician-led care for chronic diseases: A systematic review. Worldviews on Evidence-Based Nursing, 20(4), 389 to 399.
Watson, J. (2021). Caring science as sacred science. F.A. Davis.
About the Author
Dan Palmer, MSN, RN is a nursing professional and healthcare educator specializing in advanced practice nursing role transition, APRN workforce policy, and the intersection of quality measurement and professional identity development. He works with MSN students navigating the transition from expert RN to autonomous advanced practice clinician.
Connect with Dan on LinkedIn.
This guide was developed to support MSN560 students at United States University and advanced practice nurses at all stages of their professional transition. All clinical and policy information should be verified against current institutional policies, state Nurse Practice Acts, and qualified academic advisors.