
Blog
MSN560 Transitions in Practice: The Role of the Advanced Practice Nurse | Complete Expert Guide
MSN560 Transitions in Practice: The Role of the Advanced Practice Nurse
If you are enrolled in MSN560 Transitions in Practice: The Role of the Advanced Practice Nurse at United States University, or if you are navigating the early stages of an APRN career, you are standing at one of the most consequential intersections in professional nursing. You are no longer the bedside expert others defer to. You are now the clinician who bears final diagnostic and legal accountability. That shift is not merely academic. It changes how you think, how you communicate, how you carry risk, and ultimately, how you define yourself.
This guide synthesizes the full arc of that transition: the regulatory architecture that governs it, the competencies that define it, the interprofessional dynamics that complicate it, and the professional identity work that ultimately sustains it. Whether you are preparing for a course discussion, writing your Access, Cost, and Quality paper, or simply trying to make sense of what advanced practice actually demands, this is the resource you need.
What “Transition” Really Means at the Advanced Practice Level

The word “transition” appears so frequently in nursing literature that it risks losing its precision. In the context of the APRN role, transition describes something far more destabilizing than acquiring new clinical skills. It describes the simultaneous dismantling and reconstruction of a professional identity.
Patricia Benner’s Novice-to-Expert framework is widely cited in undergraduate nursing education to explain how a new graduate progresses toward clinical mastery. What is rarely discussed is what happens when that expert, a seasoned ICU nurse with twelve years of high-acuity experience, for example, enrolls in an MSN program and re-enters practice as an APRN. Benner’s model applies in reverse. The expert becomes a novice again. Not because she lacks clinical judgment, but because the scope of responsibility has fundamentally changed.
An APRN is not simply an RN with a graduate degree. The RN’s accountability was always mediated, by the physician’s orders, the care plan, the institutional protocol. The APRN’s accountability is primary. When a nurse practitioner assesses a patient with chest pain and rules out ACS, there is no attending physician who ultimately “owns” that decision. The NP owns it. That shift from mediated to primary accountability is the central psychological challenge of the APRN transition, and it is one that no amount of classroom preparation fully resolves before the first independent patient encounter.
A 2023 systematic review published in the International Journal of Nursing Studies synthesized qualitative research on this transition and found that advanced practice nurses consistently described “vague feelings and a lack of confidence in practice” even after completing their graduate education (Liu et al., 2023). This is not a competence problem. It is a role integration problem, the clinical knowledge exists, but the behavioral and psychological infrastructure for deploying it under primary accountability takes time, mentorship, and deliberate professional development to solidify.
The MSN560 course at United States University exists precisely to accelerate that infrastructure. Its focus on historical and contemporary contexts, role development theory, legal issues, prescriptive authority, and professional ethics is not a collection of disconnected topics. It is a scaffolded architecture for building the professional identity and regulatory literacy that advanced practice demands.
Understanding this from the outset, before Week 1 discussions, before the Access, Cost, and Quality paper, before the Watson Signature Assignment, changes how you engage with every module.
The Four APRN Roles: Clinical Identities, Not Just Checkboxes
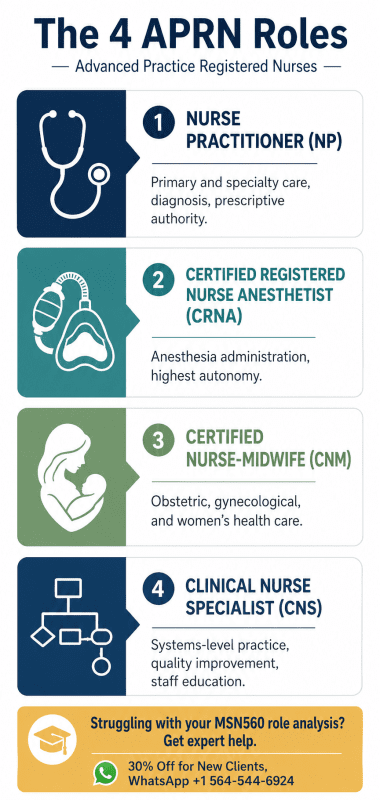
The APRN Consensus Model defines four recognized roles: the Nurse Practitioner (NP), the Certified Registered Nurse Anesthetist (CRNA), the Certified Nurse-Midwife (CNM), and the Clinical Nurse Specialist (CNS). Most survey courses treat these as four bullet points to memorize. Advanced practice demands something more: an understanding of how each role creates a distinct clinical identity, faces distinct transition challenges, and carries distinct legal and professional obligations.
Nurse Practitioner (NP)
The NP is arguably the most visible APRN role in public discourse. NPs evaluate patients, diagnose conditions, order and interpret diagnostic studies, initiate and manage treatment plans, and, depending on state law, prescribe controlled substances and practice independently. The NP is differentiated from other providers not merely by legal authority but by a nursing philosophy of care: holistic assessment, patient education, and population-level thinking are built into the NP’s clinical identity in ways that distinguish the role from physician practice even when the clinical tasks overlap.
For the transitioning NP, the most challenging competency to develop is differential diagnosis reasoning. An RN assesses; an NP diagnoses. That cognitive shift, from “these findings suggest a problem” to “this is my clinical diagnosis with these supporting and refuting findings, and here is my evidence-based management plan”, is the primary developmental task of the first year of NP practice.
Certified Registered Nurse Anesthetist (CRNA)
CRNAs administer anesthesia and related care to patients undergoing surgical, obstetric, and other procedures. They are among the highest-paid and most autonomous APRNs, and they face a distinct transition challenge: their scope is highly technical, procedurally intensive, and often immediately life-or-death in its consequences. The CRNA’s transition involves not only role identity reconstruction but also the development of near-instantaneous clinical judgment under conditions of profound patient vulnerability.
CRNAs practicing in full practice authority states do so without anesthesiologist supervision, a legislative reality that continues to generate professional conflict and political opposition from organized medicine (American Association of Nurse Anesthetists [AANA], 2022).
Certified Nurse-Midwife (CNM)
CNMs provide prenatal, intrapartum, postpartum, and gynecological care. They are uniquely positioned at the intersection of primary care and specialty obstetric practice, and they are a critical part of the solution to the United States’ maternal mortality crisis, particularly in rural and underserved communities where obstetricians are scarce. The CNM’s transition involves navigating both a highly medicalized birth culture and the philosophical legacy of midwifery as a woman-centered, low-intervention model of care.
Clinical Nurse Specialist (CNS)
The CNS is the most frequently misunderstood APRN role, and arguably the most underutilized. CNSs are systems-level change agents. They do not primarily practice at the bedside; they design, implement, and evaluate clinical programs; they mentor staff nurses; they drive quality improvement; they translate research into practice. For the transitioning CNS, the challenge is articulating value in an institutional environment that defaults to measuring provider worth in RVUs and patient throughput. The CNS’s contributions are often diffuse, indirect, and long-term, which makes them no less essential and considerably harder to defend to administrators who want metrics.
All four roles share the six population foci established by the Consensus Model: family/individual across the lifespan, adult-gerontology, pediatrics, neonatal, women’s health/gender-related, and psychiatric/mental health. Practicing outside your certified population focus is not a scope-of-practice gray area, it is a legal exposure that no malpractice carrier will cover comfortably (National Council of State Boards of Nursing [NCSBN], 2022).
The APRN Consensus Model (LACE) as Your Professional GPS
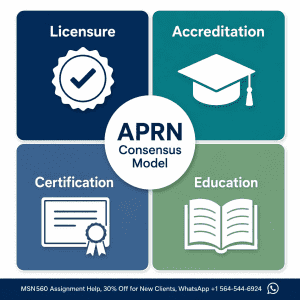
The Consensus Model for APRN Regulation: Licensure, Accreditation, Certification, and Education, universally abbreviated as LACE, was published by the NCSBN in 2008 and endorsed by over 40 nursing organizations. It remains the foundational regulatory framework governing advanced practice nursing in the United States. For MSN560 students, the Consensus Model is not background noise. It is the operating system your entire career runs on.
Licensure
Licensure is granted by individual state boards of nursing and authorizes you to practice in that state in your specific APRN role and population focus. This is where the regulatory fragmentation of American healthcare becomes immediately personal: an APRN licensed in Texas cannot simply begin practicing in New Mexico, even if both states theoretically recognize the same role. Each state has its own Nurse Practice Act, its own scope-of-practice statutes, and its own collaborative agreement requirements.
The APRN Compact, a multistate licensure agreement modeled on the existing RN licensure compact, is specifically designed to address this fragmentation. As of 2025, the Compact has gained significant momentum, and its expansion is directly tied to the LACE framework’s goal of consistent role recognition and standardized licensure across states (Philips, 2026). For new APRNs who may move, practice via telehealth across state lines, or seek employment flexibility, understanding the current status of the APRN Compact in your state is a practical first-year priority.
Accreditation
Accreditation of your graduate nursing program is the upstream variable that determines your downstream eligibility. Specifically, APRN certification bodies require that your program be accredited by either the Commission on Collegiate Nursing Education (CCNE) or the Accreditation Commission for Education in Nursing (ACEN). If your program is not accredited by one of these bodies, you may be ineligible to sit for national certification examinations, which means you cannot be licensed, which means you cannot practice.
This sounds obvious, but it has real-world consequences: students who enroll in non-CCNE/ACEN programs, perhaps attracted by cost or convenience, sometimes discover this barrier only after graduation. Verify your program’s accreditation status before enrollment, not after.
Certification
National certification validates that you have met the knowledge and competency standards for your specific APRN role and population focus. For nurse practitioners, the two primary certifying bodies are the American Association of Nurse Practitioners (AANP) and the American Nurses Credentialing Center (ANCC). Both are nationally recognized, but they differ in their examination philosophies, renewal requirements, and specialty scope.
The choice of certifying body is consequential. Some states have specific certification requirements, a handful require certification through a particular body for state licensure. Some health systems have privileging preferences. Some specialty populations (e.g., psychiatric-mental health NP) have only one recognized certification pathway. Research this before you sit for your boards, not after.
Certification is not a one-time achievement. It requires ongoing continuing education and periodic recertification. In an era of rapidly evolving clinical evidence and expanding APRN legislation, the requirement for recertification is not a bureaucratic inconvenience, it is a patient safety mechanism.
Education
The education component of LACE specifies that APRN programs must prepare graduates in one of the four recognized roles and within at least one of the six population foci. The 2021 AACN Essentials update, formally titled “The Essentials: Core Competencies for Professional Nursing Education”, restructured nursing education around competency-based outcomes rather than credit-hour accumulation, with significant implications for how MSN programs design their curricula and how students demonstrate mastery (American Association of Colleges of Nursing [AACN], 2021).
For MSN560 students, the educational component of LACE is most directly relevant when considering where to pursue additional specialization, how to evaluate continuing education offerings, and how to mentor or advise junior colleagues navigating program selection.
The Legislative Landscape: Full Practice Authority and What It Means for Your Career
No aspect of advanced practice nursing has more direct career impact, and generates more politically charged professional conflict, than the question of full practice authority. Understanding this landscape is not optional for an MSN560 student. It is a professional literacy requirement.
The Three-Tier Framework
The American Association of Nurse Practitioners (AANP) classifies state practice environments into three categories:
Full Practice Authority (FPA): State law permits APRNs to evaluate patients, diagnose, order and interpret diagnostic tests, and initiate and manage treatments, including prescribing medications and controlled substances, under the exclusive authority of the state board of nursing, without physician oversight or collaborative agreement requirements.
Reduced Practice Authority: APRNs can practice in most elements of their role but must maintain a collaborative agreement with a physician for at least one component, typically prescriptive authority.
Restricted Practice Authority: APRNs require physician supervision or collaborative agreements for the majority of their clinical functions.
The 2025 Watershed
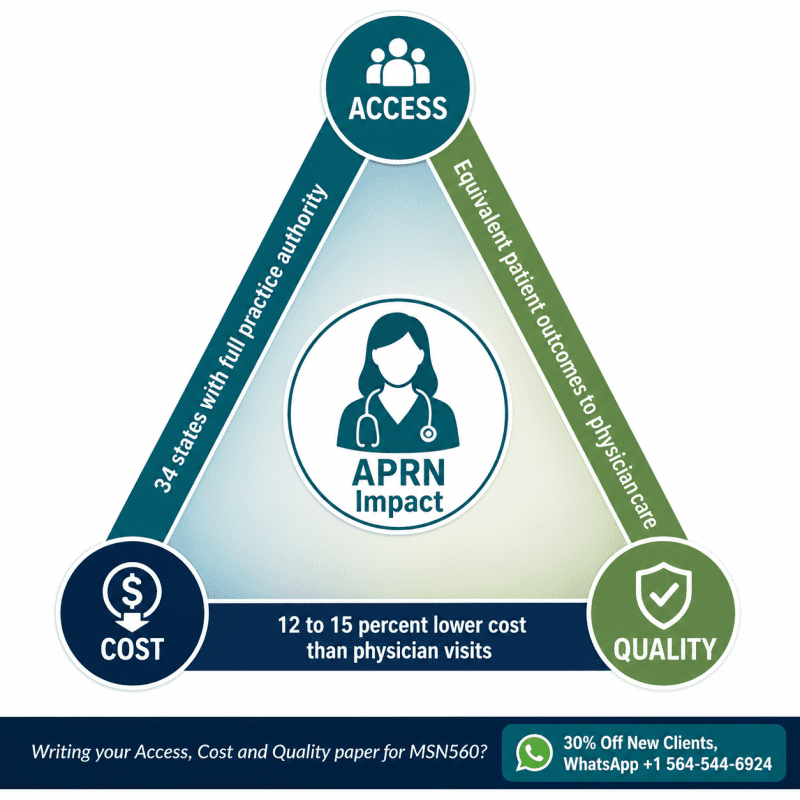
The legislative momentum toward FPA accelerated dramatically in 2025. Five states, Michigan, Alabama, Louisiana, South Carolina, and Wisconsin, enacted FPA legislation, bringing the national total to 34 states plus the District of Columbia (The HJN Blog, 2025). California, which passed Assembly Bill 890 in 2020, continued its phased implementation with full independent practice authority expected to be complete by 2026 (Phillips, 2026).
As of early 2026, 28 states and the District of Columbia grant full practice authority, with states such as New Hampshire, Rhode Island, North Dakota, South Dakota, New Mexico, and Washington among those allowing full practice immediately upon licensure (NPHub, 2026). The remaining states are at various stages of legislative debate.
The Transition-to-Practice Hour Requirement
A significant point of contention in current APRN policy is the transition-to-practice (TTP) hour requirement, a mechanism by which some states grant FPA only after an APRN completes a specified number of supervised practice hours post-graduation. Pennsylvania’s pending legislation requires 3,600 supervised hours, the longest such requirement proposed by any state (The HJN Blog, 2025).
Proponents argue that TTP requirements create a structured onboarding period that supports quality and safety. Opponents argue that they function primarily as a political compromise that delays access to care without evidence-based justification. A 2025 analysis published using National Practitioner Data Bank data found no statistically significant difference in adverse action reports or malpractice payment reports between NPs practicing in states with TTP requirements and those without, a finding with significant implications for the policy debate (Geller et al., 2025).
The Financial Reality
The practice authority landscape has direct income implications. NPs in full practice authority states earn an average of 12 to 15% more than those in restricted states, even after controlling for cost of living and experience (NursePractitionerOnline.com, 2025). Beyond income, FPA determines your ability to open an independent practice, obtain NPI billing credentials as a solo provider, serve rural and underserved populations without physician infrastructure, and practice via telehealth across jurisdictional lines.
For MSN560 students completing the Week 4 discussion on state APN practice privileges and prescriptive authority, understanding why your state sits where it sits, the political history, the organized opposition, the evidence base, is the difference between a discussion post that recites facts and one that demonstrates genuine professional analysis.
Core Competencies Every APN Must Demonstrate in Transition
The MSN560 course learning outcomes map directly onto the competency domains that define advanced practice readiness. These are not abstract academic constructs. They are the clinical, professional, and ethical capabilities that distinguish a fully transitioned APRN from one who has completed graduate coursework but not yet internalized the role.
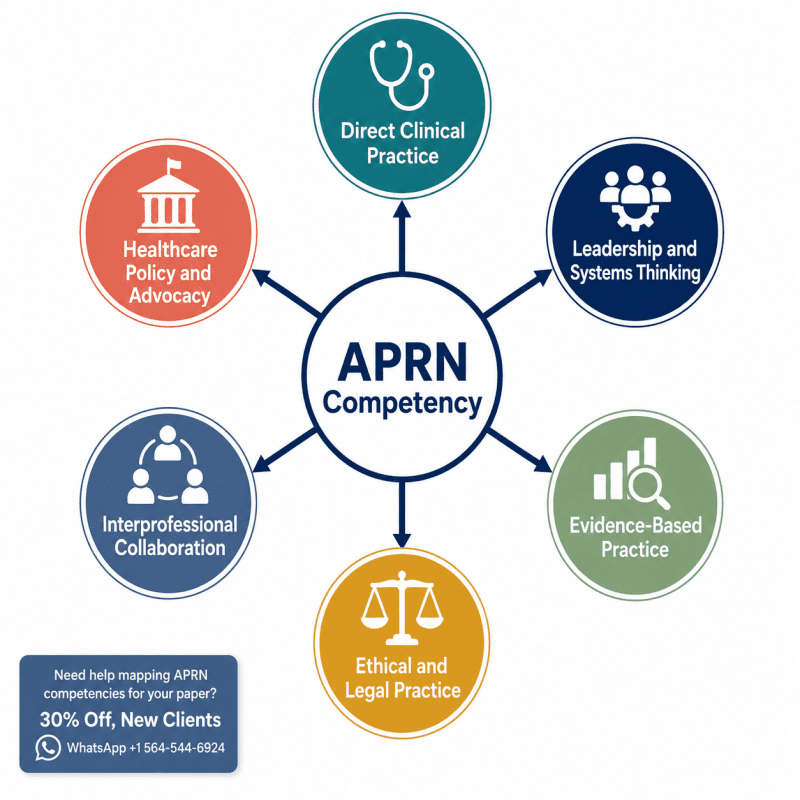
Direct Clinical Practice: The Diagnostic Imperative
Advanced health assessment in the APRN role goes beyond the comprehensive physical examination most RNs learned in their undergraduate programs. APRN-level assessment includes the systematic generation and testing of differential diagnoses, clinical reasoning under diagnostic uncertainty, and the integration of history, physical findings, diagnostic data, and patient-specific contextual factors into a coherent clinical impression and management plan.
The most common failure mode in early APRN practice is not misdiagnosis, it is premature closure: latching onto the first plausible diagnosis without adequately testing alternatives. Developing the habit of always asking “what else could this be, and what finding would help me distinguish?” is a clinical discipline that separates safe autonomous practice from supervised practice that happens to be operating without a supervisor.
Pharmacological Authority and Prescriptive Responsibility
Prescriptive authority is among the most consequential and most scrutinized aspects of APRN practice. For transitioning APRNs, the prescribing relationship with patients involves not just pharmacological knowledge but informed consent, patient education, monitoring obligations, and the legal documentation that protects both patient and provider.
Particular attention is warranted in the prescribing of controlled substances. The Drug Enforcement Administration (DEA) grants Schedule II–V prescribing authority to APRNs with the appropriate state authorization and DEA registration. The opioid prescribing crisis has made prescribing practices in this area subject to heightened regulatory and legal scrutiny, and APRNs who prescribe opioids without adequate documentation of appropriate indication, monitoring, and patient agreements face real legal exposure (Joel, 2018, Chapter 6).
Leadership: From Bedside Advocate to Systems Change Agent
The leadership competency in advanced practice is not about becoming a manager. Most APRNs in clinical roles will never manage a department. The leadership imperative is about influencing: influencing clinical protocols, influencing institutional policy, influencing legislative outcomes, and influencing the colleagues and trainees who work alongside you.
This is a competency that requires deliberate cultivation. The instinct of most transitioning APRNs is to focus on clinical excellence and leave institutional dynamics to others. That instinct, while understandable, is professionally costly. APRNs who do not engage with organizational and policy processes do not change them, and those processes will change the conditions of their practice regardless.
Evidence-Based Practice and Research: The RN-to-APN Cognitive Shift
One of the most important, and least discussed, transitions in advanced practice nursing is the shift in relationship to evidence. An RN is primarily a consumer of evidence-based practice (EBP): she implements the protocols, guidelines, and care plans that EBP generates. An APRN is expected to be a generator, translator, and evaluator of evidence.
This distinction is not merely semantic. It shapes how an APRN approaches clinical uncertainty, how she communicates with colleagues and patients, and how she contributes to quality improvement at the institutional level.
From Consumer to Critical Appraiser
In the RN role, encountering an unfamiliar clinical situation typically prompts the question: “What does the protocol say?” In the APRN role, the appropriate question is: “What does the evidence say, and does the available evidence apply to this patient in this context?” That shift requires the ability to rapidly evaluate study design, assess internal and external validity, identify confounders, and translate probabilistic population-level findings into individual patient care decisions.
MSN560 addresses this through readings in evidence-based practice (Joel, Chapter 13) and the advanced practice nurse’s role in research (Joel, Chapter 16). The Week 3 discussions on Nurse Leaders, Nurse Educators, and the Nurse Practice Act in your state provide direct opportunities to apply this critical appraisal lens to real legislative and institutional contexts.
Quality Improvement vs. Research: Knowing Which One You’re Doing
A practical point that causes significant confusion for transitioning APRNs: quality improvement (QI) and research are not the same activity, and conflating them has IRB and ethical implications. QI activities are designed to improve local processes and outcomes using existing evidence. Research is designed to generate generalizable new knowledge. The distinction determines whether your project requires IRB review, whether patients need to provide informed consent, and how your findings can be disseminated (American Nurses Association [ANA], 2022).
An APRN who implements a new sepsis screening protocol and tracks outcomes is doing QI. An APRN who randomizes patients to different sepsis protocols to test which produces better outcomes is doing research. If you are uncertain which category your project falls into, the answer is: consult your institution’s IRB office before you start, not after.
The APRN as Hospital Unit Change Agent
Chapter 9 of the Joel textbook addresses participation of the advanced practice nurse in health plans and quality initiatives. This is where the competency becomes operational. APRNs in institutional settings are uniquely positioned to drive quality improvement because they have both clinical credibility (they see patients and understand the frontline reality) and academic preparation (they can evaluate evidence, design interventions, and analyze outcomes). Institutions that fail to leverage this capacity, or APRNs who fail to exercise it, are leaving significant quality improvement potential on the table.
Interprofessional Collaboration: The Transition Skill No One Teaches Explicitly
Ask any seasoned APRN what surprised her most about the transition to advanced practice, and the answer is rarely “the pharmacology was harder than I expected.” It is almost always some version of: “I didn’t expect the interprofessional dynamics to be this complicated.”
The research bears this out. A 2023 systematic review found that the negative attitudes of physician colleagues toward new APRN roles caused advanced practice nurses to “feel disturbed and lack confidence” during the transition period, and that they were “eager to receive support from mentors to strengthen the foundation of their practice” (Liu et al., 2023). This is not an individual personality problem. It is a structural consequence of an interprofessional landscape in which physician professional identity has historically been built, in part, on the subordination of nursing clinical authority.
The Physician-APRN Collaboration Spectrum
Physician-APRN working relationships exist on a spectrum that ranges from genuine partnership, characterized by mutual respect, shared clinical decision-making, and collaborative quality improvement, to coercive oversight, in which the collaborative agreement functions as a mechanism of physician control rather than a professional resource. Most transitioning APRNs will encounter arrangements somewhere along this spectrum, and navigating that landscape requires both clinical confidence and interpersonal skill.
Several practical principles apply:
Establish clinical credibility early and visibly. In a new practice environment, your colleagues, physicians, PAs, pharmacists, and nursing staff alike, are observing how you handle uncertainty. The APRN who says “I’m not sure about this finding, let me look that up and circle back” builds more credibility over time than the one who projects false confidence. Intellectual honesty is a clinical virtue, not a weakness.
Differentiate clinical disagreement from professional boundary-testing. There is a meaningful difference between a physician colleague who questions your clinical reasoning (a collegial and often helpful dynamic) and one who challenges your authority to make autonomous decisions at all (a professional boundary issue that requires a different kind of response). Learning to distinguish between these two situations, and respond appropriately to each, is a competency that develops through experience, mentorship, and sometimes very uncomfortable conversations.
Build the interprofessional network beyond medicine. Pharmacists are among the most underutilized collaborative partners for new APRNs navigating complex polypharmacy. Social workers carry expertise in community resources, social determinants of health, and care transitions that no APRN can replicate alone. Case managers have institutional knowledge about payer requirements and post-acute resources that directly affects the feasibility of your treatment plans. Building genuine working relationships with these colleagues, not just transactional interactions, materially improves your clinical effectiveness.
Cultural Competency as an Interprofessional Skill
The MSN560 Week 6 content on cultural competency (Joel, Chapter 19) is often read as a patient care topic. It is equally relevant as an interprofessional practice skill. Health systems serve patient populations whose cultural backgrounds, health beliefs, and communication styles are diverse, and so do the healthcare teams within those systems. An APRN who can navigate cultural difference with patients but fails to recognize how her own cultural assumptions shape her professional relationships has only developed half the competency.
Cultural humility, the ongoing process of self-reflection and openness to perspectives different from your own, is a more accurate descriptor of the advanced practice standard than “cultural competence,” which implies a finite destination rather than a continuous practice (Tervalon & Murray-García, 1998, as cited in Joel, 2018).
Mentorship and Preceptorship: The Transition Accelerator
If there is a single structural variable that most consistently determines whether an APRN transition goes well or poorly, the evidence points to mentorship and preceptorship quality. Not hours. Quality.
The Distinction That Matters
A preceptor is a clinical supervisor who oversees your practice during a defined training or orientation period. A mentor is a more senior professional who provides guidance, support, and professional development over a longer arc of your career. Both are valuable. They are not the same thing, and conflating them leads to under-utilizing both.
Your preceptor’s job is to ensure you develop the clinical skills, judgment, and practice patterns required for safe autonomous practice. Your mentor’s job is to help you develop the professional identity, career strategy, and resilience required for a sustained and meaningful APRN career. You need both relationships, and you should be actively cultivating both, not waiting for your institution to provide them.
Liu et al. (2023) found that “the implementation of mentorship and the mediation of interprofessional conflicts are necessary to facilitate successful role transitions.” This is not a soft recommendation. It is a research-supported structural requirement for safe and effective APRN practice development.
Finding a Mentor When One Is Not Assigned
Many practice settings do not have formal APRN mentorship programs. In that context, new APRNs must take a proactive and somewhat entrepreneurial approach to finding mentorship.
The AANP, AACN, ACNM, and AANA all have professional development resources, networking events, and specialty interest groups that facilitate mentorship connections. State-level nursing organizations often have formal mentorship matching programs. Online communities of APRN practitioners, while no substitute for a relationship with a local clinical mentor, can provide a community of practice that normalizes the challenges of the transition period and offers practical guidance from experienced clinicians.
The key insight is this: waiting for mentorship to be provided to you is a passive stance that disadvantages you professionally. Seeking it out actively, identifying the clinician whose practice most closely aligns with your professional goals, asking directly for a mentoring relationship, and approaching that relationship with clear expectations and genuine reciprocity, is the stance of a practitioner who understands that professional development is self-directed, not institutionally delivered.
Access, Cost, and Quality: The APN’s Systemic Contribution
The Week 4 MSN560 assignment asks students to address the access, cost, and quality triad as it pertains to advanced practice nursing. This is not an exercise in reciting statistics. It is an invitation to articulate the structural case for APRN practice in a healthcare system that has not always welcomed that case.
The Access Crisis APRNs Are Built to Solve
The United States faces a primary care provider shortage of significant and worsening proportions. The Association of American Medical Colleges (AAMC) projected in 2021 a shortfall of up to 48,000 primary care physicians by 2034, a gap that physician pipeline expansion alone cannot address in any realistic timeframe (AAMC, 2021). Rural communities are disproportionately affected. The Health Resources and Services Administration (HRSA) designates thousands of geographic areas as Health Professional Shortage Areas (HPSAs), and the concentration of these designations in rural and low-income communities is not coincidental, it reflects the maldistribution of physician practice that has persisted for decades.
APRNs, and nurse practitioners in particular, are structurally positioned to address this gap. They are more likely than physicians to practice in underserved settings, more likely to accept Medicaid patients, and more likely to remain in rural practice once established (Buerhaus et al., 2022). The expansion of full practice authority is not primarily a professional prestige issue. It is a public health infrastructure issue, and framing it that way, in policy conversations, in patient education, and in professional advocacy, is part of the APRN’s political literacy.
The Quality Argument: What the Evidence Actually Shows
The question of whether APRN-provided care is equivalent in quality to physician-provided care has been studied extensively, with remarkably consistent results. A systematic review published in the Cochrane Database of Systematic Reviews found no significant differences in patient health outcomes between NP-managed and physician-managed care across multiple domains, including patient satisfaction, health status outcomes, and care process measures (Laurant et al., 2018, updated 2022). Some analyses have found superior performance by NPs on preventive care metrics, a finding consistent with nursing’s historical emphasis on health promotion and patient education.
The relevant quality question for MSN560 purposes is not “are APRNs as good as doctors?” That framing concedes physician practice as the gold standard against which nursing must perpetually prove itself. The more accurate and professionally empowering question is: “What does APRN-provided care do well, for which populations, under what conditions, and how do we optimize the practice environment to maximize those outcomes?” That question directs attention toward improving APRN practice rather than defending it.
Cost-Effectiveness and Reimbursement Parity
APRN-provided care is demonstrably cost-effective relative to physician-provided care for the conditions and patient populations where the two roles overlap. APRN salaries are lower, APRN training is shorter, and the per-visit cost of APRN care in primary care settings is consistently lower than equivalent physician visits (Buerhaus et al., 2022).
The current reimbursement landscape, however, creates a structural distortion: Medicare reimburses NPs at 85% of the physician fee schedule for identical services, a differential that was justified historically by arguments about different training requirements but that is increasingly difficult to defend in an era of demonstrated outcome equivalence. The ANA and AANP have actively lobbied for reimbursement parity, framing it as both an equity issue and a healthcare access issue (ANA, 2023).
Healthcare Policy Advocacy as an APN Identity, Not an Add-On
The MSN560 Week 5 content on public policy and the advanced practice nurse (Joel, Chapters 10 and 14) frames advocacy as a professional obligation. That framing is correct, and it is worth unpacking what it means in practice.
Many APRNs arrive at graduate school with the sense that politics is someone else’s domain, that their job is to take care of patients, and advocacy is for lobbyists and professional organizations. That distinction collapses quickly when you realize that every scope-of-practice restriction you navigate, every collaborative agreement you are required to maintain, every reimbursement differential you absorb, is the direct product of a policy decision made by people who may or may not have had APRN perspectives at the table.
The 38th Annual APRN Legislative Update, published in January 2026 in The Nurse Practitioner, identified key themes in 2025 legislative changes: steps toward administrative modernization, pathways to independent prescribing, and incremental gains in reimbursement parity (Phillips, 2026). These gains did not happen because legislators spontaneously decided to expand APRN authority. They happened because APRN professional organizations, individual clinicians, and patient advocacy groups showed up, to public comment periods, legislative hearings, constituent meetings, and ballot campaigns.
What Engagement Actually Looks Like
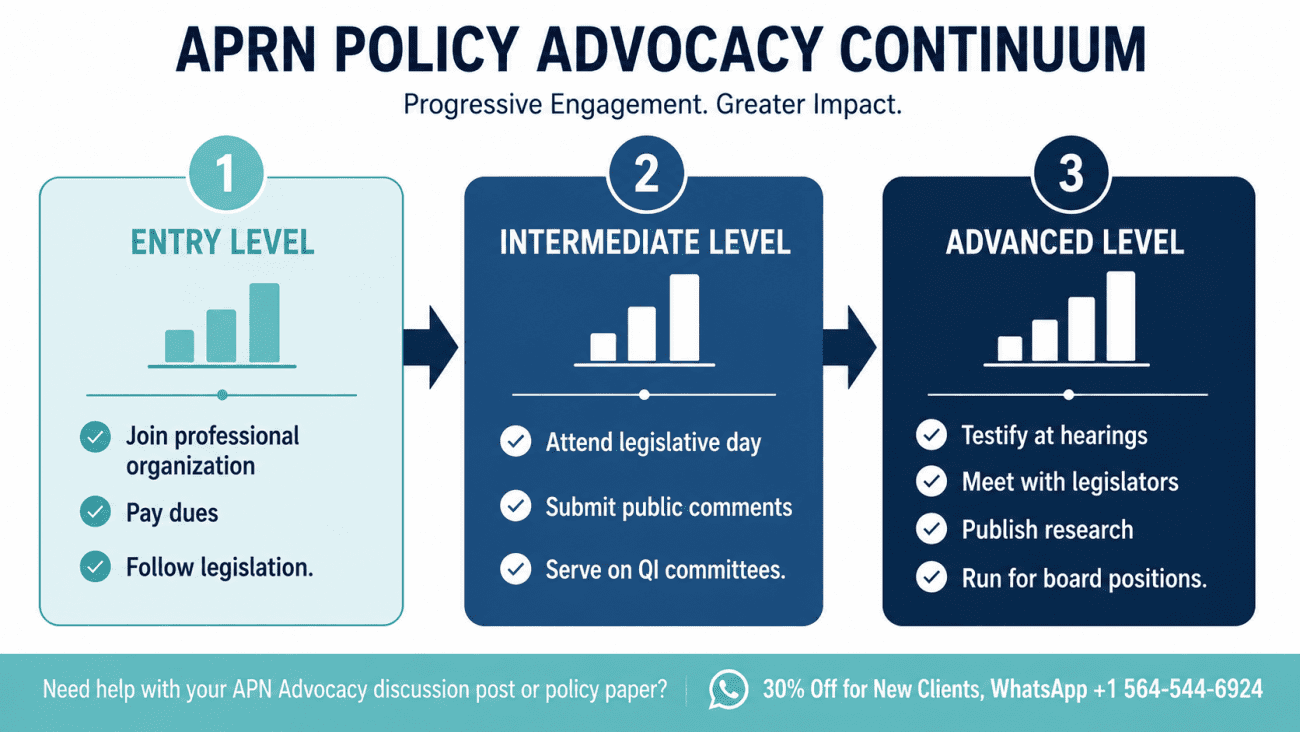
Policy engagement for the practicing APRN is not an all-or-nothing proposition. It exists on a continuum:
- At the entry level, joining your professional organization (AANP, AACN, ACNM, AANA, or your state-level affiliate) and paying dues is a form of advocacy, you are funding the organizations that employ lobbyists, conduct legislative research, and file amicus briefs.
- At the intermediate level, participating in public comment periods on proposed regulations affecting APRN practice, a process that is open to any licensed provider and requires only time and the ability to articulate your clinical perspective, is a meaningful contribution.
- At the advanced level, testifying at legislative hearings, meeting with your state legislators’ office to discuss APRN practice authority, or running for positions on your state board of nursing are forms of advocacy that have documented impact on legislative outcomes.
- For MSN560 Week 5, the APN Advocacy discussion is an opportunity to move beyond reciting the policy landscape and articulate specifically what you will do, not what APRNs should do in general, but what you, with your clinical background, your state’s legislative context, and your specific patient population, will do to advance APRN practice authority and patient access.
Jean Watson’s Theory of Human Caring in the Advanced Practice Role
The MSN560 Signature Assignment, the Week 7 PowerPoint presentation on the influence of Jean Watson’s Theory of Human Caring on your future APN role, is the capstone of the course. For many students, Watson’s theory is encountered initially as an academic framework to satisfy a course requirement. For the APRN who genuinely integrates it, it becomes something more: a professional philosophy that sustains ethical practice across the inevitable challenges and moral distresses of advanced clinical care.
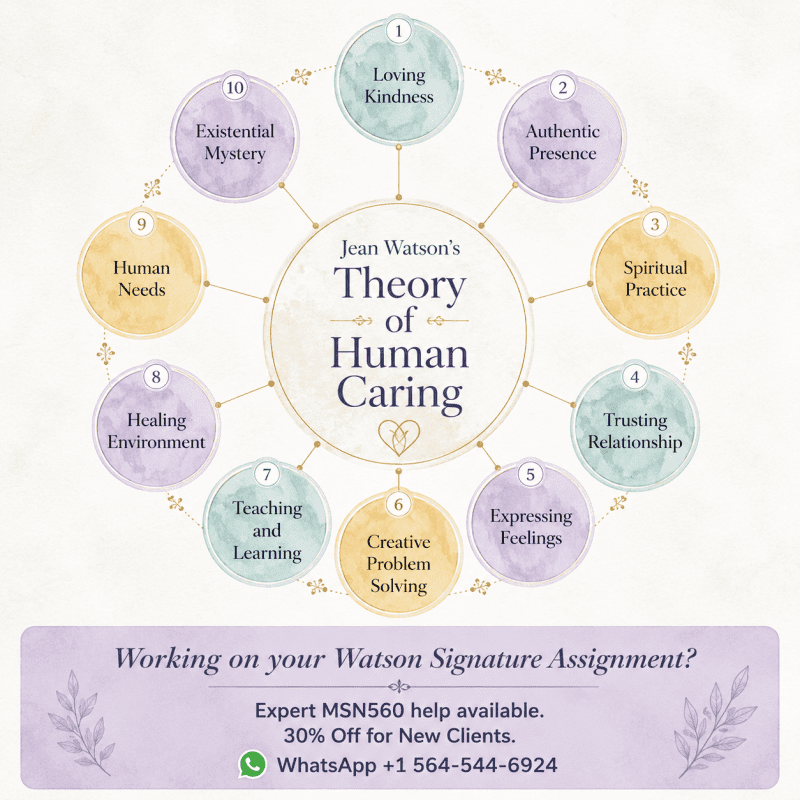
Core Concepts and the Ten Caritas Processes
Watson’s theory centers on the concept of the transpersonal caring relationship, an encounter between two people in which both the caring-healer and the care-seeker are changed by the authentic connection. This is not a soft or romantic notion. It is a philosophical claim about the ontology of healthcare: that healing occurs not merely through technical interventions but through the quality of the human connection in which those interventions are embedded.
The ten Caritas Processes, Watson’s evolution of her original carative factors, provide a practical framework for implementing this philosophy in clinical practice. They include cultivating loving kindness toward self and others, instilling authentic hope, developing sensitivity to self and others, creating healing environments, and allowing for existential and spiritual dimensions of care (Watson, 2021).
For the APRN who prescribes, diagnoses, and manages complex chronic disease, the Caritas Processes are not decorative additions to the clinical encounter. They are the framework that keeps the clinician from reducing the patient to a problem to be solved. In a healthcare system that incentivizes throughput, measures quality in metrics, and increasingly interposes electronic documentation between clinician and patient, Watson’s theory is a professional counterweight, a reminder that the person in the exam room is not a bundle of diagnoses but a human being whose experience of illness, whose fears about the future, and whose relationships and values are as clinically relevant as her laboratory results.
Watson’s Theory in the MSN560 Curricular Context
The course structures Watson’s theory as the philosophical through-line of the curriculum: Week 1 introduces Jean Watson’s core concepts and asks students to apply them to APN practice; Week 7’s Signature Assignment asks students to synthesize that application into a professional presentation. Between those bookends, every clinical topic in the course, interprofessional collaboration, cultural competency, conflict resolution, resource management, gains additional depth when read through the lens of caring science.
The APRN who approaches a conflicted interprofessional relationship with the Caritas Process of “practicing being present and supportive of the expression of positive and negative feelings” will navigate that conflict differently than one who approaches it purely as a political or professional power negotiation. The APRN who brings loving kindness toward self as well as others to the realities of moral distress in clinical practice will sustain her professional engagement differently than one who depletes herself in service of others without cultivating reciprocal self-compassion.
Watson’s theory is not naive. It does not ask APRNs to pretend that clinical practice is uniformly beautiful or that human connection always heals. It asks APRNs to hold the reality of suffering with intention, with presence, and with the conviction that caring itself is a clinical act. That is not a soft skill. That is the philosophical foundation of advanced practice.
Telehealth, AI, and the Evolving APN Scope
The APRN transition today occurs in a practice environment that is qualitatively different from the one that produced the Consensus Model in 2008 and the Joel textbook in 2018. Two developments, in particular, are reshaping the operational reality of advanced practice: telehealth expansion and the integration of artificial intelligence into clinical workflows.
Telehealth and Multi-State Practice
The COVID-19 pandemic forced a rapid and largely successful expansion of telehealth across healthcare settings, and many of the emergency waivers that enabled that expansion, including waivers of the requirement that providers be licensed in the patient’s state, have become subjects of permanent legislative debate. For APRNs, telehealth creates a practice environment in which the geographic boundaries of a license become operationally relevant in new ways.
An NP licensed in Texas who sees a patient via telehealth who is physically located in New Mexico at the time of the encounter is, under most current state interpretations, practicing in New Mexico and subject to New Mexico’s Nurse Practice Act. If New Mexico requires a collaborative agreement for prescriptive authority and Texas does not, the telehealth NP is operating under the more restrictive framework during that encounter.
The APRN Compact is specifically designed to address this complexity, and its adoption timeline is a practical consideration for any APRN planning to incorporate telehealth into her practice (NCSBN, 2022).
Artificial Intelligence in Clinical Decision Support
AI-assisted clinical decision support tools are increasingly embedded in electronic health record systems, diagnostic platforms, and patient communication technologies. For APRNs, these tools create both opportunity and new categories of professional responsibility.
The opportunity is genuine: AI that flags potential drug-drug interactions, identifies sepsis risk scores, or surfaces relevant clinical literature during the patient encounter can meaningfully support APRN clinical judgment, particularly for new graduates still developing the pattern recognition that accrues with clinical experience.
The professional responsibility is equally genuine: AI clinical decision support tools reflect the biases, limitations, and population characteristics of the data on which they were trained. An APRN who accepts an AI recommendation without applying clinical judgment has not augmented her practice, she has delegated it. The legal standard for APRN practice requires that clinical decisions be made by the licensed provider, not by the algorithm. Understanding when to use, when to question, and when to override AI recommendations is a new competency that current APRN programs are only beginning to address systematically.
Information Technology and the APN (Joel, Chapter 22)
The MSN560 Week 7 reading on information technology and the advanced practice nurse covers EHR utilization, clinical informatics, and telehealth from a practice management perspective. The key application for transitioning APRNs is documentation: the EHR is simultaneously your primary clinical tool, your billing record, your legal defense document, and your quality metric generator. Documentation that is clinically thorough, accurately coded, and contemporaneously completed is not a clerical task, it is a professional obligation with direct implications for patient safety, institutional revenue, and malpractice defense.
Legal, Ethical, and Malpractice Considerations for the Transitioning APN
The MSN560 Week 8 modules on law, ethics, and malpractice (Joel, Chapters 27 to 30) are among the most practically consequential in the course. They are also among the most anxiety-provoking for students who are confronting, perhaps for the first time, the legal reality of autonomous clinical practice.
Scope Creep: The Most Common Legal Risk
Scope creep, practicing beyond your certified scope without the clinical education, certification, or legal authorization to support that practice, is the most common legal exposure for transitioning APRNs. It typically does not begin with a dramatic decision to perform an unauthorized procedure. It begins with small, incremental expansions in response to institutional need, patient request, or physician colleague expectation.
The clinical test is straightforward: if your graduate program did not educate and supervise you in a particular clinical competency, and your certification does not cover it, and your state Nurse Practice Act does not authorize it, you should not be performing it, regardless of who is asking. This is not timidity. It is professional integrity and patient safety practice.
Independent Contractor vs. Employee: Legal and Contractual Implications
The Week 8 discussion on APNs as employees versus independent contractors (Joel, Chapter 27) has direct financial and legal implications that many new graduates are unprepared for. Employment as an APRN in a healthcare system typically means the employer carries malpractice insurance, defines your scope of practice via institutional credentialing, and controls the terms of your clinical work. Independent contracting means you are responsible for your own malpractice coverage, your own professional credentialing, your own billing infrastructure, and your own contract negotiation.
Neither arrangement is inherently superior. Each carries advantages and obligations that must be carefully evaluated against your specific practice goals, risk tolerance, and career stage. The guidance of a healthcare attorney before signing any APRN employment or independent contractor agreement is money well spent.
Malpractice: Understand It Before You Need It
APRN malpractice liability is governed by the same legal standard that governs all healthcare providers: the reasonable provider standard, what would a similarly trained and experienced APRN have done in the same or similar circumstances? The standard is not perfection. It is competent, evidence-based practice with appropriate documentation.
Malpractice insurance is non-negotiable for any independently practicing APRN. Even APRNs employed by health systems who are covered under institutional policies should consider individual coverage, institutional policies protect the institution’s interests, not necessarily yours. Occurrence-based coverage (which covers any incident that occurred during the policy period, regardless of when the claim is filed) is generally preferable to claims-made coverage (which covers only claims filed while the policy is active) for the long-term professional (Joel, 2018, Chapter 29).
Starting a Practice and Practice Management
For APRNs with entrepreneurial ambitions, or for those in underserved communities where building an independent practice may be the only way to provide needed care, the Week 7 content on practice management (Joel, Chapter 26) introduces the operational and financial realities of APRN business ownership.
Starting an independent APRN practice requires facility with domains that graduate nursing programs rarely cover in depth: business planning, legal entity formation, credentialing with payers, billing and coding, human resources, real estate, and marketing. The transition from clinician to clinician-entrepreneur is itself a form of role transition, one that reactivates many of the same identity reconstruction challenges that characterized the RN-to-APRN transition.
Resource Management in Primary Care
The Week 7 Discussion 2 on resource management in primary care engages a reality that clinical training can obscure: the delivery of healthcare requires the efficient allocation of finite resources, clinical staff time, diagnostic equipment, medication formularies, referral relationships, and payer contracts, in a way that maximizes both patient outcomes and organizational sustainability. An APRN who is clinically excellent but financially illiterate is a practice liability in any setting.
Understanding the revenue cycle, the relationship between diagnostic coding accuracy and reimbursement, the cost implications of clinical decisions, and the regulatory requirements for practice operations is not a betrayal of nursing’s caring ethos. It is the infrastructure that makes sustained, high-quality caring practice possible.
Building Your Professional Identity as an APN
The synthesis of everything discussed in this guide ultimately comes back to a question of identity: who are you becoming as an advanced practice nurse?
That question is not merely rhetorical. A 2023 systematic review found that professional role transitions involve “a dynamic process in which individuals develop new identities, values, and knowledge bases,” and that “the role development of advanced practice nurses can be affected by environmental, organisational and social factors” (Liu et al., 2023). Your professional identity as an APRN is not fixed at graduation. It is actively constructed, through every clinical encounter that challenges your judgment, every interprofessional conflict that tests your professional boundaries, every policy advocacy effort that expands your understanding of where your practice fits in the larger system.
The Role Grief No One Mentions
Many transitioning APRNs experience what might be called professional role grief: a genuine sense of loss for the expert RN identity they are leaving behind. The bedside nurse who knew her unit like the back of her hand, who every colleague trusted in a code, who patients and families called by first name and hugged on discharge, that clinician is not who she is anymore. She is a novice again, and the psychological adjustment to that reality is real and legitimate.
Naming this experience, rather than dismissing it as weakness or ingratitude for the advanced practice opportunity, is a clinical and personal health practice. Nurses, particularly those who ascend to advanced practice, are socialized to minimize their own needs and absorb whatever the clinical environment demands. That socialization is a professional liability, and confronting it honestly is part of what Watson’s caring science framework, applied to self as well as to patients, actually requires.
Your Personal Philosophy of Practice
The Signature Assignment’s invitation to explore Watson’s influence on your future APN role is, at its deepest level, an invitation to begin articulating your personal philosophy of practice. What do you believe about the purpose of healthcare? What do you believe about the therapeutic relationship? What do you believe about your obligations to the communities you serve, not just the individuals in your exam room, but the population whose health your practice pattern will cumulatively affect?
A personal philosophy of practice is not a document you write once and file. It is a living orientation that you revisit as your experience deepens, as your patient population changes, and as the healthcare system around you evolves. APRNs who practice with an articulated philosophy tend to navigate moral distress, professional conflict, and career transitions with more resilience than those who do not, not because the philosophy protects them from difficulty, but because it gives them a frame within which difficulty makes sense.
MSN560 Synthesis: Connecting Course Concepts to Real Practice
The eight-week structure of MSN560 is not arbitrary. It builds from foundational role development theory in Week 1 to the legal and ethical capstone of Week 8, with the Watson Signature Assignment at Week 7 functioning as the integrative centerpiece. Here is how the major course threads connect:
Role Development Theory (Week 1) → Leadership (Week 2): You cannot lead a role you have not conceptually inhabited. Benner’s model, Watson’s philosophy, and the emerging roles literature provide the intellectual foundation for the leadership content that follows.
Emerging Roles and Healthcare Trends (Week 2) → Legislative Landscape (Week 3 to 4): Understanding what APRNs can do is inseparable from understanding what the law currently permits them to do, and what advocacy is required to align the two.
LACE and Prescriptive Authority (Week 4) → Access, Cost, Quality (Week 4): The regulatory architecture of APRN practice exists in service of a goal: improving population health through expanded access to high-quality, cost-effective care. The LACE framework makes sense when read in that functional context.
Policy and Advocacy (Week 5) → Collaboration and Conflict (Week 6): Policy is not made in a vacuum. The interprofessional conflicts that shape daily APRN practice are the microcosm of the macroscopic policy conflicts that shape the regulatory environment. Developing skills in both arenas is a unified professional development project.
Watson Signature Assignment (Week 7) → Ethics and Law (Week 8): Watson’s caring philosophy provides the ethical orientation within which the legal frameworks of Week 8 operate. An APRN who understands why ethical practice matters, not just what the law requires, practices at a level of professional integrity that legal compliance alone does not guarantee.
Frequently Asked Questions: MSN560 and the Advanced Practice Nurse Role
About MSN560 and the Course
What is MSN560 Transitions in Practice: The Role of the Advanced Practice Nurse?
MSN560 is a 3-credit graduate nursing course offered at United States University as part of its Master of Science in Nursing program. The course addresses the role and accountabilities of advanced practice nurses across historical and contemporary contexts. It covers role development theory, leadership, certification, prescriptive authority, ethics, legal issues, interprofessional collaboration, healthcare policy, and the influence of Jean Watson’s Theory of Human Caring on the APN role. The course runs eight weeks and culminates in a Signature Assignment, a presentation applying Watson’s caring science to the student’s future APN role. It requires no prerequisites and serves as a foundational course for the MSN program.
What are the major assignments in MSN560?
MSN560 includes eight weekly discussion boards (two per week, 16 total), eight quizzes drawn from the Joel textbook chapters, a Plagiarism Exercise and APA Scavenger Hunt in the early weeks, an Access, Cost, and Quality paper (1,500 words, Week 4), an APN Infographic (Week 5), a Virtual Class with the Librarian (Week 2), and the Signature Assignment, a PowerPoint presentation on the Theory of Human Caring in your future APN role (Week 7, 250 points, 25% of grade). The course uses the Joel Advanced Practice Nursing: Essentials for Role Development (4th ed.) as its primary textbook.
What is the required textbook for MSN560?
The required textbook is Joel, L.A. (2018). Advanced Practice Nursing: Essentials for Role Development (4th ed.). F.A. Davis Company. ISBN-13: 978-0-8036-6044-1. The course also requires the APA Publication Manual (7th ed.) for formatting all written assignments.
What are the course learning outcomes for MSN560?
Upon completion of MSN560, students should be able to: (1) discuss traditional and emerging APRN roles in response to healthcare trends at local, state, national, and global levels; (2) analyze historical and contemporary issues of education, titling, certification, and licensure; (3) explore the functional roles of APNs, clinician, educator, researcher, administrator, entrepreneur, consultant, and leader; (4) debate the policies, social, financial, legal, and ethical issues in advanced practice nursing; and (5) evaluate the influence of Jean Watson’s Theory of Human Caring on the advanced practice role.
About the APRN Transition to Practice
What does “transition to practice” mean for an advanced practice nurse?
Transition to practice in the APRN context refers to the period during which a newly credentialed advanced practice nurse moves from supervised graduate clinical training into independent or semi-independent professional practice. This transition involves more than learning new clinical skills, it requires rebuilding a professional identity. An APRN is no longer an expert RN whose clinical decisions are mediated by physician orders and institutional protocols. She bears primary diagnostic and legal accountability for her patients. That shift, from mediated to primary accountability, is the central psychological and professional challenge of the APRN transition, and research consistently shows it takes 12 to 24 months of mentored practice to fully integrate (Liu et al., 2023).
How long does the APRN transition to practice typically take?
The formal transition period varies by state and employment setting. In states with transition-to-practice (TTP) hour requirements, the supervised period is defined in statute, ranging from approximately 2,000 hours in some states to 4,600 hours in others (e.g., California’s pathway to independent NP practice). Beyond the legal definition, research indicates that most APRNs do not report full confidence in their role until 12 to 24 months after entering independent practice. Factors that significantly accelerate the transition include access to high-quality mentorship, a practice environment with supportive interprofessional relationships, and deliberate engagement with continuing professional development.
What is the biggest challenge APRNs face during role transition?
Based on the clinical literature, the most consistently reported challenge is not clinical knowledge deficits, it is the psychological and professional identity reconstruction required by the role shift. APRNs transitioning from RN practice frequently report vague feelings of inadequacy and a lack of confidence, even when their clinical performance is objectively sound (Liu et al., 2023). A second major challenge is navigating interprofessional dynamics: physician colleagues who resist APRN clinical authority, institutional credentialing processes that do not reflect the APRN’s full scope of practice, and the absence of formal mentorship in many practice settings.
What is the difference between an RN and an APRN in terms of clinical accountability?
An RN functions within a mediated accountability structure: her clinical decisions are implemented within a care plan that is ultimately ordered by a licensed prescriber (typically a physician), and her professional obligations are defined by the institutional protocols, care plans, and standing orders within which she operates. An APRN bears primary clinical accountability. A nurse practitioner, for example, conducts the assessment, generates the differential diagnosis, orders and interprets the diagnostic studies, makes the diagnosis, and initiates and manages the treatment plan, including prescribing medications, under her own licensure and professional authority. There is no physician who “owns” that chain of decisions. The APRN owns it.
About APRN Roles and the Consensus Model
What are the four APRN roles recognized by the Consensus Model?
The APRN Consensus Model (NCSBN, 2008) recognizes four roles: (1) the Nurse Practitioner (NP), who provides primary and specialty care including diagnosis, treatment, and prescriptive management; (2) the Certified Registered Nurse Anesthetist (CRNA), who administers anesthesia and peri-anesthesia care; (3) the Certified Nurse-Midwife (CNM), who provides obstetric, gynecological, and women’s health care; and (4) the Clinical Nurse Specialist (CNS), who functions as a systems-level advanced practice clinician, educator, and change agent. Each role requires graduate-level education, national certification, and state licensure in that specific role and within at least one of the six recognized population foci.
What are the six population foci in the APRN Consensus Model?
The six population foci are: (1) family/individual across the lifespan, (2) adult-gerontology, (3) pediatrics, (4) neonatal, (5) women’s health/gender-related, and (6) psychiatric/mental health. APRNs must be educated, certified, and licensed within a specific role and at least one population focus. Practicing outside your certified population focus is a scope-of-practice violation and a significant legal and malpractice exposure, not a gray area.
What does LACE stand for, and why does it matter for transitioning APRNs?
LACE stands for Licensure, Accreditation, Certification, and Education, the four regulatory pillars of the APRN Consensus Model. Licensure is the state-granted legal authorization to practice in your role and population focus. Accreditation ensures your graduate program meets national standards recognized by certification bodies. Certification validates your role-specific clinical competency through national examination.
Education defines the graduate-level preparation required for each APRN role and population focus. LACE matters to transitioning APRNs because each pillar has direct, practical implications: the wrong program accreditation can make you ineligible for national certification; practicing without the correct state licensure is illegal; letting your certification lapse may require you to requalify rather than simply renew.
What is the Clinical Nurse Specialist (CNS) role, and how does it differ from the NP?
The CNS is the most frequently misunderstood APRN role. While NPs primarily provide direct patient care, diagnosing, treating, and prescribing, CNSs function primarily as systems-level advanced practice clinicians. Their work spans three spheres of impact: the patient/family sphere (direct care for complex patients), the nursing/staff sphere (staff education, mentorship, and practice development), and the organizational/systems sphere (program design, quality improvement, and clinical protocol development). CNSs typically do not carry independent patient panels in the way NPs do. Their value is often diffuse and long-term, which makes them harder to justify in RVU-driven institutional cultures, and no less essential for it.
About Full Practice Authority and State Law
What states have full practice authority for nurse practitioners in 2025 to 2026?
As of 2026, 28 states plus the District of Columbia grant full practice authority (FPA) to nurse practitioners, allowing them to evaluate patients, diagnose, order and interpret diagnostic tests, and prescribe medications, including controlled substances, without physician oversight or collaborative agreement requirements. States with FPA include New Hampshire, Rhode Island, North Dakota, South Dakota, New Mexico, Washington, Oregon, Montana, and others.
Five additional states, Michigan, Alabama, Louisiana, South Carolina, and Wisconsin, enacted FPA legislation in 2025, bringing the national total of FPA states to 34 at the broadest count (including states with transition-period provisions). California continues its phased implementation with full independent practice expected to be complete by 2026 (NPHub, 2026; The HJN Blog, 2025).
What is the difference between full, reduced, and restricted practice authority?
Full practice authority (FPA) means APRNs can practice to the full extent of their education and certification under the exclusive authority of the state board of nursing, no physician oversight or collaborative agreement required. Reduced practice authority means APRNs can practice most clinical functions independently but must maintain a collaborative agreement with a physician for at least one component, typically prescriptive authority. Restricted practice authority requires physician supervision or collaborative agreements for the majority of clinical functions.
The category your state falls into determines your clinical autonomy, your ability to open an independent practice, your telehealth billing eligibility, and, according to recent data, your earning potential, with NPs in FPA states earning 12 to 15% more on average than those in restricted states (NursePractitionerOnline.com, 2025).
What is a transition-to-practice (TTP) hour requirement?
A transition-to-practice (TTP) hour requirement is a legislative mechanism used by some states to grant full practice authority only after a new APRN has completed a specified number of supervised clinical hours following graduation and initial licensure. The requirement ranges from approximately 2,000 to 4,600 hours across states. Proponents argue TTP requirements provide a structured onboarding that supports patient safety. Critics, supported by a 2025 National Practitioner Data Bank analysis, argue there is no statistically significant association between TTP hour requirements and reduced adverse action reports or malpractice claims, suggesting these requirements function more as political barriers to practice than as safety mechanisms (Geller et al., 2025).
Can an APRN practice across state lines via telehealth?
Generally, yes, but only if the APRN holds a valid license in the state where the patient is physically located at the time of the encounter. A telehealth visit does not exempt an APRN from the licensure requirements of the patient’s state. The APRN Compact, modeled on the existing RN licensure compact, is designed to streamline this by creating a multistate licensure mechanism that allows qualified APRNs to practice across compact member states under a single license. As of 2025, the Compact has expanded significantly in adoption, but not all states are members. APRNs integrating telehealth into their practice must verify their licensure status in every state where they see patients.
About APRN Competencies, Ethics, and Scope
What is scope creep in APRN practice, and why is it dangerous?
Scope creep occurs when an APRN practices clinical activities that fall outside her certified scope of practice, beyond what she was educated and supervised in during her graduate program, covered by her national certification, and legally authorized to perform under her state’s Nurse Practice Act. It rarely begins dramatically; it typically starts with small, incremental expansions in response to institutional pressure, patient requests, or physician colleague expectations.
Scope creep is dangerous because it removes the APRN from the coverage of her malpractice insurance, exposes her to state board disciplinary action, and, most importantly, places patients in the care of a provider who lacks the specific competency that clinical situation requires. The professional standard is clear: if your graduate education, national certification, and state law do not authorize it, do not do it.
What is the standard of care for APRN malpractice liability?
The standard of care in APRN malpractice cases is the reasonable provider standard: what would a similarly trained and experienced APRN have done under the same or similar clinical circumstances? This is not a perfection standard. It is a competent, evidence-based practice standard. APRNs are not held to the physician standard of care, nor to the RN standard, they are held to the APRN standard for their specific role and population focus. Documentation is central to malpractice defense: contemporaneous, clinically thorough, accurately coded documentation that reflects your clinical reasoning, informed consent discussions, patient education, and follow-up plans is your primary legal protection.
What is Jean Watson’s Theory of Human Caring, and how does it apply to APN practice?
Jean Watson’s Theory of Human Caring is a nursing philosophy centered on the transpersonal caring relationship, an authentic human connection between clinician and patient in which healing occurs not solely through technical intervention but through the quality of the caring encounter itself. Watson’s ten Caritas Processes provide a practical clinical framework: they include cultivating loving kindness toward self and others, practicing authentic presence, developing sensitivity to self and others, creating healing environments, and allowing for the spiritual and existential dimensions of care (Watson, 2021).
For APRNs, Watson’s theory provides a professional counterweight to a healthcare system that incentivizes throughput and measures quality in metrics, a philosophical foundation that keeps the person in the exam room from being reduced to a bundle of diagnoses. In MSN560, Watson’s theory is the philosophical through-line of the curriculum, culminating in the Week 7 Signature Assignment.
What does the AACN 2021 Essentials mean for MSN students?
The AACN’s 2021 Essentials: Core Competencies for Professional Nursing Education represents the most significant restructuring of nursing education standards in decades. It shifts from credit-hour-based curriculum design to competency-based outcomes, organizing advanced nursing education around ten domains, including person-centered care, population health, interprofessional partnerships, clinical judgment, informatics, and nursing science. For MSN560 students, the practical implication is that courses like MSN560 are not just knowledge delivery vehicles, they are competency development frameworks. Your discussions, assignments, and clinical reflections are evidence of competency attainment, not just academic exercises.
About APRN Advocacy and the Future of the Role
How can APRNs engage in policy advocacy?
Policy engagement for the practicing APRN exists on a continuum. At the entry level, joining and paying dues to your professional organization (AANP, AACN, ACNM, AANA, or your state-level affiliate) is a tangible act of advocacy, you are funding the organizations that employ lobbyists and conduct legislative research. Participating in public comment periods on proposed regulations is open to any licensed provider and requires only time.
At the intermediate level, attending your state nursing association’s legislative day, writing to your state legislators about APRN practice authority, or serving on hospital quality improvement committees extends your advocacy reach. At the advanced level, testifying at legislative hearings, running for your state board of nursing, or contributing to peer-reviewed research on APRN outcomes creates durable systemic impact.
Why is reimbursement parity an important advocacy issue for APRNs?
Medicare currently reimburses NPs at 85% of the physician fee schedule for identical services, a differential that was originally justified by arguments about training-level differences but is increasingly difficult to defend given the body of evidence demonstrating equivalent patient outcomes for NP-managed care (Laurant et al., 2018, updated 2022). Reimbursement parity is both an equity issue, equal pay for equal work, and a healthcare access issue: the reimbursement differential creates a financial disincentive for health systems to maximize APRN practice capacity, which directly reduces the workforce available to serve underserved communities. The ANA and AANP continue to actively advocate for full reimbursement parity at the federal level (ANA, 2023).
What are the emerging roles for APRNs in the current healthcare landscape?
The MSN560 Week 2 content on emerging APRN roles (Joel, Chapter 2) reflects a rapidly evolving practice landscape. Current emerging and expanding roles include: Telehealth NPs and CNSs practicing across state lines under the APRN Compact; Hospitalist NPs managing complex inpatient populations with limited physician availability; Psychiatric Mental Health NPs (PMHNPs) addressing the national mental health provider shortage; APRN Entrepreneurs establishing independent practices in underserved communities; Palliative Care APRNs providing specialist-level symptom management and goals-of-care support; and Informatics-focused APRNs bridging clinical practice and healthcare technology design.
The common thread across these emerging roles is expanded autonomy, expanded accountability, and the consistent need for the professional development infrastructure that MSN560 is designed to provide.
References
American Association of Colleges of Nursing. (2021). The essentials: Core competencies for professional nursing education. https://www.aacnnursing.org/Portals/42/AcademicNursing/pdf/Essentials-2021.pdf
American Association of Nurse Anesthetists. (2022). CRNA fact sheet. https://www.aana.com/membership/become-a-crna/crna-fact-sheet
American Association of Nurse Practitioners. (2023). NP fact sheet. https://www.aanp.org/all-about-nps/np-fact-sheet
American Nurses Association. (2022). Nursing: Scope and standards of practice (4th ed.). ANA.
American Nurses Association. (2023). Reimbursement parity for APRNs. https://www.nursingworld.org/practice-policy/health-policy/
Association of American Medical Colleges. (2021). The complexities of physician supply and demand: Projections from 2019 to 2034. AAMC.
Buerhaus, P. I., Skinner, L. E., Auerbach, D. I., & Staiger, D. O. (2022). State of the registered nurse workforce as a new era of health care delivery emerges. Nursing Economic$, 40(2), 58 to 71.
Geller, A. I., Derman, R. J., Havranek, E. P., & Lichtenstein, A. H. (2025). Do transition to practice hour requirements make a difference in adverse action and medical malpractice payment reports: An analysis from the National Practitioner Data Bank. Journal of the American Association of Nurse Practitioners. https://pmc.ncbi.nlm.nih.gov/articles/PMC12118611/
Joel, L. A. (2018). Advanced practice nursing: Essentials for role development (4th ed.). F.A. Davis.
Laurant, M., van der Biezen, M., Wijers, N., Watananirun, K., Kontopantelis, E., & van Vught, A. J. (2018, updated 2022). Nurses as substitutes for doctors in primary care. Cochrane Database of Systematic Reviews, (7), CD001271.
Liu, Y., Yang, J., Liu, H., Zhang, W., & Huang, L. (2023). The transition to advanced practice nursing: A systematic review of qualitative studies. International Journal of Nursing Studies, 143, Article 104491. https://doi.org/10.1016/j.ijnurstu.2023.104491
National Council of State Boards of Nursing. (2022). APRN Consensus Model toolkit. https://www.ncsbn.org/aprn-consensus-model-toolkit
NPHub. (2026, March). Understanding the nurse practitioner scope of practice across states. https://www.nphub.com/blog/np-scope-practice-state
NursePractitionerOnline.com. (2025, October). Nurse practitioner practice authority 2025: Complete state-by-state analysis. https://www.nursepractitioneronline.com/articles/nurse-practitioner-practice-authority-updates/
Phillips, S. J. (2021, January). 33rd annual APRN legislative update: Unprecedented changes to APRN practice authority in unprecedented times. The Nurse Practitioner, 46(1), 27 to 55.
Phillips, S. J. (2026, January). 38th annual APRN legislative update: Transformative change through APRN practice authority progress. The Nurse Practitioner. https://nursing.uci.edu/news-events
The HJN Blog. (2025, May). State-by-state guide: Expanding roles for PAs and NPs (updated 2025). https://blog.healthjobsnationwide.com/state-by-state-guide-expanding-roles-for-pas-and-nps-updated-2025/
Watson, J. (2021). Caring science as sacred science. F.A. Davis.
19. About the Author
Dan Palmer, MSN, RN is a nursing professional and healthcare educator with extensive clinical and academic experience in advanced practice nursing. His work focuses on the preparation and development of advanced practice nurses navigating the transition from expert RN to autonomous clinical provider, with particular interest in APRN workforce policy, interprofessional practice, and caring science as a framework for sustainable clinical leadership.
Connect with Dan on LinkedIn.