The psychiatric interview components and the Beck Depression Inventory-II (BDI-II)

Psychiatric Interview Components & BDI-II: A PMHNP Evidence-Based Guide
| Direct Answer to Main Discussion Question:
The three core components of the psychiatric interview — the Chief Complaint and History of Present Illness (HPI), the Psychiatric History, and the Mental Status Examination (MSE) — are the foundational pillars every PMHNP relies on to diagnose, formulate, and treat psychiatric conditions. When paired with a validated evidence-based rating scale such as the Beck Depression Inventory-II (BDI-II), these components produce a comprehensive, measurement-informed psychiatric assessment that exceeds the accuracy of clinical judgment alone. The BDI-II’s strong psychometric properties, including Cronbach’s alpha of 0.86–0.92 and confirmed bifactor validity, make it the gold standard self-report depression scale in outpatient PMHNP practice. |
What Are the Three Most Important Components of the Psychiatric Interview?
The psychiatric interview has three non-negotiable components: the Chief Complaint and HPI, the Psychiatric History, and the Mental Status Examination. Each component serves a distinct diagnostic function — none can be omitted without compromising clinical accuracy.
Psychiatric mental health nurse practitioners (PMHNPs) use these three domains to build a complete picture of the patient’s illness, from the patient’s subjective experience to objective clinical signs, contextualized within a longitudinal history.
Component 1: What Is the Chief Complaint and Why Does It Matter?
The chief complaint is the patient’s verbatim statement — recorded in quotation marks — of why they sought psychiatric care. It is the diagnostic anchor of every clinical encounter and must never be paraphrased or clinically interpreted by the PMHNP before it is documented.
This single sentence does more diagnostic work than any questionnaire. A patient who states ‘I haven’t left my house in three weeks’ communicates functional impairment, duration, and severity simultaneously.
What Should the History of Present Illness (HPI) Include?
The HPI elaborates the chief complaint across onset, duration, severity, precipitating and alleviating factors, and associated symptoms. It is not a template — it is a clinical narrative that places the patient’s current suffering in meaningful context.
The PMHNP explores how symptoms have evolved, what has worsened or improved the patient’s condition, and what functional domains have been affected — sleep, work, relationships, self-care.
- Onset and duration: When did symptoms begin? Were there identifiable triggers?
- Severity: How does this episode compare to any prior episodes in intensity and function?
- Associated symptoms: Anxiety, psychosis, substance use, sleep and appetite disturbance, suicidal ideation.
- Suicidality: Ideation, intent, plan, means access — assessed within the HPI, not as a separate checklist.
Why Is Suicidal Ideation Assessment Part of the HPI — Not a Separate Step?
Embedding suicidal ideation assessment within the HPI — rather than as a disconnected screener — produces more accurate clinical data and deepens therapeutic alliance. The American Psychiatric Association (2022) confirms that direct questioning about suicide does not increase risk; it opens critical dialogue.
A patient who is asked about suicidality within the natural flow of their illness narrative is more likely to disclose. Asking the same question on a disconnected checklist decontextualizes risk and may yield underreporting.
| Evidence Pearl:
The APA (2022) states that passive suicidal and homicidal thoughts are common, and discussion can often lead to a deepening of the alliance. Manualized suicide assessment tools are increasingly integrated alongside the HPI in mental health settings and primary care. |
Component 2: Why Is the Psychiatric History a Diagnostic Game-Changer?
The psychiatric history shifts the PMHNP’s diagnostic reasoning from cross-sectional pattern recognition to longitudinal illness conceptualization. A patient who appears to have a first major depressive episode may have an undisclosed hypomanic history that changes the diagnosis — and the treatment — entirely.
Sadock, Sadock, and Ruiz (2021) define the psychiatric history as the context that contrasts current findings with past treatment and illness episodes, providing perspective that no single-visit assessment can replicate.
What Must a Comprehensive Psychiatric History Include?
- Past psychiatric diagnoses: DSM-5 diagnoses, prior hospitalizations, prior medication trials and responses, adverse effects experienced.
- Substance use history: Type, frequency, quantity, last use, history of withdrawal, and substance-related psychiatric sequelae.
- Family psychiatric history: First-degree relatives with mood disorders, psychosis, suicides, or substance dependence — critical for diagnostic and prognostic reasoning.
- Social and developmental history: Trauma exposure, adverse childhood experiences (ACEs), educational attainment, occupational functioning, and relationship patterns.
- Legal history: Relevant to risk stratification, commitment considerations, and forensic psychiatric overlap.
How Does the Psychiatric History Prevent Diagnostic Error?
Diagnostic error in psychiatry most often occurs when the PMHNP relies solely on the current presentation without interrogating the longitudinal record. A patient screened for depression who has a prior manic episode, a family history of bipolar disorder, and a history of antidepressant-induced hypomania requires a fundamentally different clinical formulation.
The psychiatric history is not bureaucratic form-filling. Every item carries weight. A remote hospitalization at age 22 may be more diagnostically informative than the current chief complaint.
Component 3: What Does the Mental Status Examination Actually Assess?
The Mental Status Examination (MSE) is the systematic, clinician-administered assessment of the patient’s current mental functioning across 10 domains. Unlike the HPI and psychiatric history — which are retrospective — the MSE is a real-time objective snapshot of the patient’s mental state during the encounter.
Voss and Das (StatPearls, 2024) confirm that the MSE begins the moment the patient enters the clinical setting — through observation of gait, dress, psychomotor behavior, and interactions with staff — before a single structured question is asked.
What Are the 10 Domains of the Mental Status Examination?
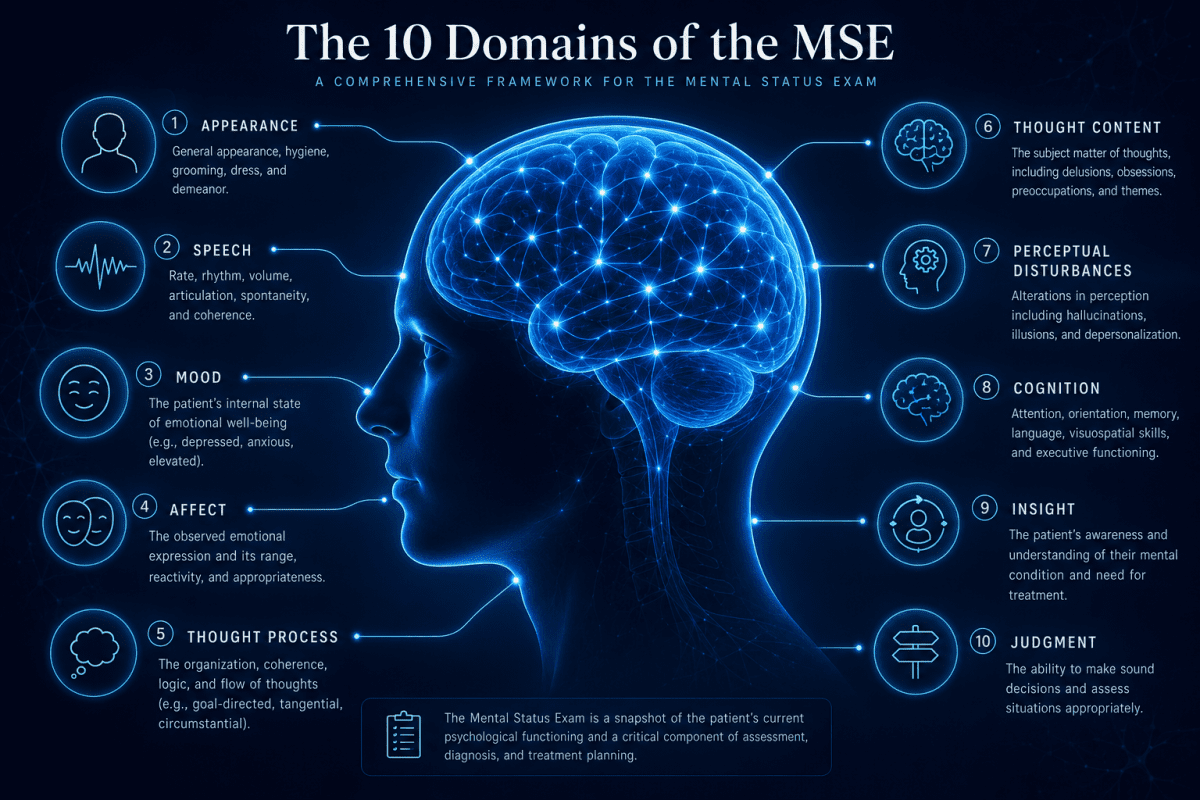
- Appearance — grooming, dress, hygiene, posture, age-appropriateness
- Behavior and psychomotor activity — agitation, retardation, abnormal movements
- Speech — rate, rhythm, volume, latency, spontaneity
- Mood — patient’s subjective, self-reported emotional state (in quotes)
- Affect — clinician-observed emotional expression: range, intensity, congruence
- Thought process — linear, circumstantial, tangential, loose associations, flight of ideas
- Thought content — suicidal ideation, homicidal ideation, delusions, obsessions, phobias
- Perceptual disturbances — hallucinations (auditory, visual, tactile), illusions, depersonalization
- Cognition — orientation, attention, memory, abstract reasoning, fund of knowledge
- Insight and judgment — awareness of illness; ability to make reasoned, safe decisions
What Is the Difference Between Mood and Affect in the MSE?
Mood is what the patient reports feeling; affect is what the clinician observes. This distinction is diagnostically critical, not semantic.
A patient with major depression may report ‘fine’ while demonstrating restricted affect, psychomotor retardation, and a flattened vocal tone throughout the interview. The discrepancy between stated mood and observed affect is clinically significant data.
Incongruent affect — such as laughing while discussing a plan to self-harm — carries immediate risk implications and must be documented and addressed in the assessment.
Why Can the MSE Not Be Replaced by a Self-Report Scale?
The MSE captures objective, observed clinical signs that no patient self-report instrument can replicate. A patient minimizing symptoms due to stigma, impression management, or anosognosia will nonetheless reveal psychomotor slowing, thought blocking, or loose associations to a trained clinician.
This is why the MSE and a validated rating scale like the BDI-II are complementary data sources — one captures what the patient observes about themselves; the other captures what the clinician observes about the patient.
What Is the Beck Depression Inventory-II (BDI-II)?
The Beck Depression Inventory-Second Edition (BDI-II) is a 21-item, validated self-report instrument that quantifies the presence and severity of depressive symptoms in adults and adolescents aged 13 and older, aligned with DSM-5 diagnostic criteria. Total scores range from 0 to 63; higher scores indicate greater depressive symptom severity.
Developed by Aaron T. Beck and colleagues and revised in 1996 to align with updated diagnostic criteria, the BDI-II assesses cognitive, affective, and somatic dimensions of depression across 21 items completed by the patient in approximately 5–10 minutes.
The BDI-II is one of the most widely used and psychometrically validated depression rating instruments globally, appearing in peer-reviewed research across more than 50 countries and language groups (Cogan, Persons, & Kring, 2023; Fernandez-Castilla et al., 2023).
What Do the 21 BDI-II Items Assess?
The BDI-II covers the full DSM-5 depressive symptom spectrum across three factor domains:
- Cognitive domain: Sadness, pessimism, past failure, self-dislike, self-criticalness, worthlessness, indecisiveness, loss of interest, suicidal thoughts
- Affective domain: Crying, agitation, loss of pleasure, irritability
- Somatic domain: Loss of energy, sleep changes, appetite changes, concentration difficulty, fatigue, loss of interest in sex
| Clinical Note:
Item 9 directly assesses suicidal ideation. Any score of 1 or above on Item 9 — regardless of the total BDI-II score — requires immediate PMHNP clinical follow-up, full suicide risk assessment, documentation, and safety planning or escalation of care. |
What Are the Psychometric Properties of the BDI-II?
The BDI-II demonstrates strong psychometric properties across reliability, validity, factor structure, and cultural equivalence. These properties collectively qualify it as a gold-standard self-report instrument for depression severity in PMHNP clinical practice.
| Psychometric Property | Key Finding | Clinical Significance |
|---|---|---|
| Internal Consistency | α = 0.86–0.92 | Items reliably measure the same depression construct across diverse populations |
| Test-Retest Reliability | r = 0.73–0.96 | Stable scores support longitudinal treatment monitoring across visits |
| Convergent Validity | High correlation with HAM-D and PHQ-9 | Aligns with established depression measures, confirming diagnostic utility |
| Discriminant Validity | Distinguishes depression from anxiety | Reduces false-positive MDD diagnosis in patients with primary anxiety disorders |
| Factor Structure | Bifactor: general depression + cognitive, affective, somatic | Enables subscale interpretation for targeted treatment planning |
| Cross-Cultural Validity | Validated in 50+ countries/languages | Appropriate for multicultural PMHNP patient populations (Fernandez-Castilla et al., 2023) |
| Sensitivity to Change | Detects clinically significant symptom shifts | Ideal for measurement-based care and tracking pharmacotherapy/therapy response |
What Do BDI-II Scores Mean Clinically?
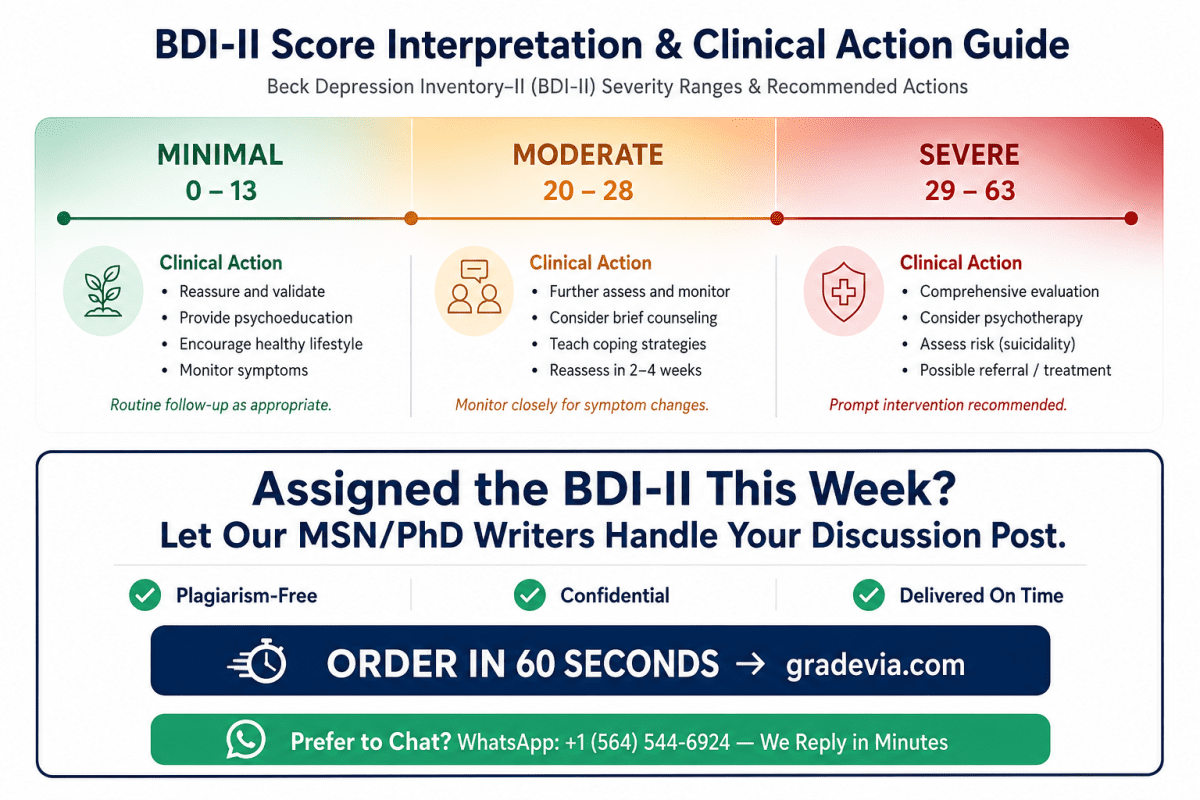
BDI-II total scores map to four validated severity classifications that guide clinical decision-making:
| Score | Severity Classification & Clinical Implication |
|---|---|
| 0 – 13 | Minimal Depression — Monitor; reassess if functional decline occurs |
| 14 – 19 | Mild Depression — Psychotherapy initiation, watchful waiting, close follow-up |
| 20 – 28 | Moderate Depression — Pharmacotherapy and/or structured psychotherapy strongly indicated |
| 29 – 63 | Severe Depression — Urgent intervention; assess need for higher level of care |
How Does the BDI-II’s Bifactor Structure Aid Clinical Decision-Making?
The bifactor model — with a general depression factor and three specific subscales (cognitive, affective, somatic) — allows the PMHNP to interpret the pattern of depression, not just the severity. This distinction directly informs treatment selection.
A patient whose BDI-II profile is dominated by cognitive items — pessimism, worthlessness, self-criticalness, past failure — is a stronger candidate for cognitive-behavioral therapy than pharmacotherapy alone.
Conversely, a patient whose scores cluster in somatic items — fatigue, sleep disturbance, appetite change, loss of libido — may respond more robustly to antidepressant pharmacotherapy as a first-line intervention (Cogan et al., 2023).
When Is It Appropriate to Use the BDI-II During the Psychiatric Interview?
The BDI-II is clinically appropriate whenever a patient presents with a chief complaint of depressed mood, anhedonia, low energy, or neurovegetative symptoms — or when treatment response monitoring is required across sequential visits. Timing and sequencing within the encounter matter.
What Are the Specific Clinical Indications for BDI-II Administration?
- New-onset depression presentation: Quantifies baseline symptom severity to anchor the treatment formulation and set measurable recovery targets.
- Prior history of depressive episodes: Re-establishes severity at current visit; enables comparison to prior episode data.
- Comorbid medical illness with known depression prevalence: Post-MI depression, Parkinson’s disease, post-stroke depression, cancer-related depression — populations where somatic symptoms overlap significantly with depressive symptoms.
- Ongoing pharmacotherapy or psychotherapy: Tracks treatment response visit-to-visit; identifies non-response or partial response early.
- Diagnostic ambiguity: Quantifies symptom severity when verbal report is minimized, unreliable, or culturally modulated.
Should the BDI-II Be Administered Before or After the Clinical Interview?
Both approaches have evidence-based rationale; the PMHNP’s decision should be driven by clinical context.
Pre-interview administration allows the clinician to review item-level responses before the structured assessment begins. This primes clinical attention to the most endorsed symptoms — particularly Item 9 — and enables individualized, targeted questioning rather than a generic symptom review.
Post-interview administration allows the BDI-II to serve as a structured quantification of what the patient has already narrated, providing a numeric anchor for documentation and treatment planning. Patients who verbalize distress comfortably may find this sequence more natural.
When Is the BDI-II NOT Appropriate?
- Active psychotic disorders or acute manic episodes — where self-report accuracy is unreliable
- Significant cognitive impairment that compromises reliable self-completion
- Low literacy — an oral administration with clinician-read items can mitigate this limitation
- As a standalone diagnostic instrument — the BDI-II quantifies severity; it does not diagnose MDD
How Does the BDI-II Strengthen the PMHNP’s Psychiatric Assessment?
The BDI-II strengthens the PMHNP’s psychiatric assessment by providing four clinically measurable advantages over unaided interview alone: quantified baseline, longitudinal tracking, elicitation of underreported symptoms, and subscale-level treatment guidance.
What Is Measurement-Based Care and Why Does It Matter?
Measurement-based care (MBC) is the systematic administration of validated clinical rating scales at every encounter to inform treatment decisions, track symptom trajectory, and detect deterioration before it becomes clinically visible. Torous and Keshavan (2023) identify MBC as demonstrating consistent superiority over unaided clinical judgment in depression treatment outcomes.
The BDI-II is the most practical entry point to MBC in depression management — brief, psychometrically robust, and sensitive to clinically meaningful change across visits.
| Evidence:
Torous and Keshavan (2023, JAMA Psychiatry) found that measurement-based care significantly improves depression treatment outcomes compared to unaided clinical assessment. The BDI-II’s sensitivity to change makes it particularly effective as a MBC instrument in outpatient PMHNP settings. |
How Does the BDI-II Complement — Not Replace — the MSE?
The MSE captures what the clinician observes; the BDI-II captures what the patient experiences. These are fundamentally different data sources that each capture clinically significant information invisible to the other.
A patient with a relatively unremarkable MSE — due to emotional blunting, impression management, or a transient good day — may score in the severe range on the BDI-II, revealing a symptom burden invisible to observation alone.
Conversely, a patient with an agitated, tearful MSE presentation may score in the moderate range on the BDI-II if the current episode is brief and has not yet generalized. Neither source is complete without the other.
How Does the BDI-II Capture Symptoms That Patients Underreport?
Somatic and sexual symptoms of depression are consistently underreported in verbal psychiatric interviews — patients either attribute them to general medical causes or are reluctant to raise them spontaneously.
The BDI-II’s structured item format prompts direct endorsement of fatigue, sleep disturbance, appetite change, and loss of libido, ensuring these symptom domains enter the diagnostic and treatment formulation regardless of patient reticence.
Clinical Practice Tips: Maximizing the Psychiatric Interview and BDI-II
How Should PMHNPs Record the Chief Complaint?
Always record the chief complaint verbatim, in the patient’s exact words, in quotation marks. The patient’s illness language is diagnostically informative; clinical paraphrase strips away meaning.
What Are the Most Diagnostically Rich MSE Domains?
Thought content, affect-mood congruence, and insight/judgment carry disproportionate diagnostic and risk management weight. Never abbreviate these domains under time pressure.
How Should PMHNPs Handle BDI-II Item 9 Endorsement?
Any Item 9 score of 1 or greater triggers mandatory full suicide risk assessment — regardless of total BDI-II score. Document the specific ideation, the clinical reasoning, the safety plan or escalation decision, and the plan for follow-up.
How Often Should the BDI-II Be Repeated?
In measurement-based care, the BDI-II should be administered at every clinical encounter — including medication management visits — to enable meaningful visit-to-visit comparison. A 50% reduction in total score is a commonly used threshold for clinically significant treatment response.
What Is the PMHNP’s Role When MSE and BDI-II Results Diverge?
Divergence between the MSE and BDI-II is not a data error — it is a clinical signal. When a patient presents with a benign MSE but a high BDI-II score, probe for minimization, impression management, or between-session worsening that is not captured in the interview moment.
Frequently Asked Questions (People Also Ask)
Q: What are the three most important components of the psychiatric interview?
The three most important components are: (1) the Chief Complaint and History of Present Illness, (2) the Psychiatric History, and (3) the Mental Status Examination. Together these generate the subjective, historical, and objective data required for a DSM-5 diagnosis and individualized treatment plan. No single component is sufficient alone.
Q: What is the difference between the BDI and the BDI-II?
The BDI-II (1996) is the updated second edition of Beck’s original 1961 inventory, revised to align with DSM-IV and subsequently DSM-5 diagnostic criteria. The BDI-II replaced outdated items, extended the symptom timeframe to two weeks, and added items for agitation and worthlessness. In contemporary PMHNP practice, BDI-II and BDI are used interchangeably to refer to the second edition.
Q: Can the BDI-II diagnose major depressive disorder?
No — the BDI-II is a symptom severity rating scale, not a diagnostic instrument. A score in the severe range (29+) indicates significant depressive symptom burden but does not constitute a DSM-5 diagnosis. Diagnosis requires a full psychiatric interview, MSE, differential diagnosis reasoning, and clinical judgment that accounts for medical causes, substance use, and bereavement.
Q: What is measurement-based care in psychiatric nursing?
Measurement-based care (MBC) is the systematic use of validated clinical rating scales at every encounter to guide treatment decisions, track symptom severity, and detect non-response early. Evidence demonstrates MBC produces superior depression treatment outcomes compared to unaided clinical assessment. The BDI-II is one of the most efficient MBC instruments in outpatient psychiatric nursing due to its brevity and psychometric strength (Torous & Keshavan, 2023).
Q: How does the MSE differ from a neurological examination?
The MSE is a psychiatric assessment of mental functioning — mood, affect, thought, cognition, insight, and behavior — while the neurological examination assesses structural nervous system integrity through motor, sensory, reflex, and coordination testing. The two complement each other; PMHNPs routinely incorporate cognitive screening (MMSE, MoCA) within the MSE to identify neurocognitive disorders that require neurological evaluation.
Q: What psychometric properties make the BDI-II reliable?
The BDI-II demonstrates excellent internal consistency (Cronbach’s alpha 0.86–0.92), strong test-retest reliability (r = 0.73–0.96), and confirmed convergent, discriminant, and cross-cultural validity. A bifactor model confirms the scale reliably measures a general depression construct alongside three specific subdimensions: cognitive, affective, and somatic. These properties have been replicated across more than 50 countries (Fernandez-Castilla et al., 2023).
References
American Psychiatric Association. (2022). Diagnostic and statistical manual of mental disorders (5th ed., text rev.). American Psychiatric Publishing.
American Psychiatric Nurses Association. (2024). Using the Brief Psychiatric Rating Scale (BPRS) as a symptom assessment tool in measurement-based care. APNA eLearning Center.
Beck, A. T., Steer, R. A., & Brown, G. K. (1996). Beck Depression Inventory–Second Edition manual. The Psychological Corporation.
Carlat, D. J. (2017). The psychiatric interview (4th ed.). Wolters Kluwer.
Cogan, A. B., Persons, J. B., & Kring, A. M. (2023). Using the Beck Depression Inventory to assess anhedonia: A scale validation study. Assessment, 31(1), 3–16. https://doi.org/10.1177/10731911231164628
Fernandez-Castilla, B., Declercq, L., Jamshidi, L., Beretvas, S. N., Onghena, P., & Van den Noortgate, W. (2023). Psychometric properties and cross-cultural invariance of the BDI-II and BAI among Spanish, Portuguese, and Brazilian undergraduate students. International Journal of Environmental Research and Public Health, 20(11), 6009.
Sadock, B. J., Sadock, V. A., & Ruiz, P. (2021). Kaplan & Sadock’s synopsis of psychiatry (12th ed.). Wolters Kluwer.
Springer Publishing Company. (2023). The psychiatric interview. In Psychiatric Mental Health Nurse Practitioner Review and Resource Manual (5th ed.).
Torous, J., & Keshavan, M. (2023). Measurement-based care in psychiatry: Implementation and clinical utility. JAMA Psychiatry, 80(3), 206–214. https://doi.org/10.1001/jamapsychiatry.2022.4392
Voss, R. M., & Das, J. M. (2024, April 30). Mental status examination. In StatPearls [Internet]. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK546682/
About the Author
| Dan Palmer, MSN
Dan Palmer is a professional psychiatric mental health writer with 14 years of writing practice experience in psychiatric mental health topics. He has written about various topics covering Walden University nursing courses like NRNP 6635 Psychopathology and Diagnostic Reasoning and other related graduate courses. His scholarly interests include depression screening in medically complex patients, culturally responsive psychiatric assessment, and standardized rating scale optimization in primary care psychiatry. |
© Original publication June 1, 2026. PMHNP Clinical Resource. For educational use only. Not a substitute for clinical judgment or licensed professional guidance.