Comprehensive Psychiatric Evaluation for Mood Disorders: NRNP 6635 Week 3 Assignment Guide

Comprehensive Psychiatric Evaluation for Mood Disorders
The NRNP 6635 Week 3 comprehensive psychiatric evaluation requires PMHNP students to complete a full SOAP-format assessment of a mood disorder patient, including a detailed subjective history using the GoChMP mnemonic, an objective mental status examination written in paragraph form, at least three differential diagnoses compared using DSM-5-TR criteria, and a critical reflection addressing legal, ethical, and social determinants of health. This guide walks through every section mapped to the 100-point rubric so you earn full marks on your first submission.
Assignment Instructions, Required Sources, Video links, and Grading rubric: Assessing and Diagnosing Patients With Mood Disorders
What Is a Comprehensive Psychiatric Evaluation for Mood Disorders?
A comprehensive psychiatric evaluation is a structured, evidence-based clinical document that captures the full picture of a patient’s mental health presentation — from their chief complaint to their social circumstances — in order to generate a defensible primary diagnosis and treatment plan.
For NRNP 6635 Week 3, you are specifically assessing and diagnosing patients with mood disorders — a category that includes Major Depressive Disorder (MDD), Bipolar I and II Disorder, Cyclothymic Disorder, Disruptive Mood Dysregulation Disorder (DMDD), and Persistent Depressive Disorder (dysthymia).
Mood disorders are among the most challenging psychiatric conditions to diagnose accurately. The American Psychiatric Association (2022) notes that their cyclic, periodic nature — and the overlap between depressive, manic, and mixed features — means that even experienced clinicians must follow a rigorous diagnostic process. This guide gives you that process, mapped step by step to the Walden rubric.
Why Mood Disorders Are Particularly Hard to Diagnose
Research from the Journal of Clinical Psychiatry (2022) shows that up to 65% of patients with Bipolar Disorder are initially misdiagnosed — most commonly as Major Depressive Disorder — because they present during a depressive episode and do not spontaneously report prior manic or hypomanic symptoms.
This diagnostic challenge makes the comprehensive psychiatric evaluation especially important. Your SOAP note must demonstrate that you actively screened for the full mood disorder spectrum, not just the presenting complaint.
- Depressive disorders (MDD, persistent depressive disorder, DMDD) — affect mood persistently downward
- Bipolar and related disorders (Bipolar I, II, cyclothymia) — involve mood cycling between poles
- Substance-induced mood disorders — must be ruled out in every case
- Mood disorder due to another medical condition — thyroid, neurological, and metabolic causes must be excluded
How to Select the Right Video Case Study for Week 3
The Week 3 assignment gives you nine Symptom Media training titles to choose from (Training Titles 2, 8, 18, 28, 38, 43, 118, 144, and 150). Select the case that presents the clearest mood disorder features — typically one involving episodes of depression, mood instability, irritability, or cycling — so your differential diagnosis section has the clinical richness needed for the assessment rubric’s 25-point criterion.
Training Title 18, for example, involves a patient presenting with possible PTSD and depression — a case requiring you to differentiate mood disorder from trauma-related disorder, which demonstrates strong clinical reasoning. Read the Case History Reports document in full before writing your note; it contains collateral data not visible in the video.
Pro tip: Choose your video first, take detailed notes on every symptom, and review the case history before touching the template. The video is your primary data source — the note is your clinical documentation of it.
How to Write the Subjective Section (20 Points)
The subjective section is the patient’s story in their own words, supplemented by clinician-gathered history. It earns 20 points and must be thorough, accurate, and well-organized to hit the Excellent tier.
Chief Complaint (CC): Use the Patient’s Exact Words
The chief complaint is always a verbatim quote from the patient. It is not a diagnosis and not a clinical summary. Write it as: CC: “I feel like I’m on a roller coaster and I can’t get off.”
This verbatim standard serves a clinical purpose — the patient’s own language often reveals diagnostic clues. A patient who says “I feel like electricity running through me” is describing something qualitatively different from one who says “I feel sad.”
History of Present Illness (HPI): Paint the Full Clinical Picture
Begin the HPI with the patient’s initials, age, race, gender, purpose of the evaluation, current medications, and referral source. Then conduct a psychiatric review of symptoms that covers onset, duration, frequency, severity, and functional impact.
For mood disorder patients specifically, your HPI must screen across the full spectrum:
- Depressive symptoms: SIGECAPS (Sleep disturbance, Interest loss, Guilt, Energy loss, Concentration difficulty, Appetite change, Psychomotor changes, Suicidal ideation)
- Manic/hypomanic symptoms: DIGFAST (Distractibility, Impulsivity/Indiscretion, Grandiosity, Flight of ideas, Activity increase, Sleep decrease, Talkativeness/pressured speech)
- Anxiety symptoms: to rule out GAD, panic disorder, PTSD as primary diagnosis
- Psychotic symptoms: hallucinations, delusions, thought disorganization — critical to rule out schizoaffective disorder
- Trauma history: PTSD can mimic mood instability and cycling
The exemplar standard: “Paint a picture of what is wrong with the patient.” Your HPI should read like a compelling clinical narrative — not a checkbox list.
Substance Use History: The Most Overlooked Section
Substance use history is clinically critical for mood disorder evaluations because the DSM-5-TR requires you to rule out substance-induced mood disorder before assigning any primary mood diagnosis. Document caffeine, nicotine, alcohol, cannabis, and all illicit substances.
For each substance, document: type, daily amount, last known use, route of administration, and any withdrawal history (tremors, delirium tremens, seizures). A patient who drinks heavily and presents with depressive symptoms may be experiencing alcohol-induced depression, not MDD — a diagnosis with an entirely different treatment pathway.
The GoChMP Mnemonic: Your Psychiatric History Framework
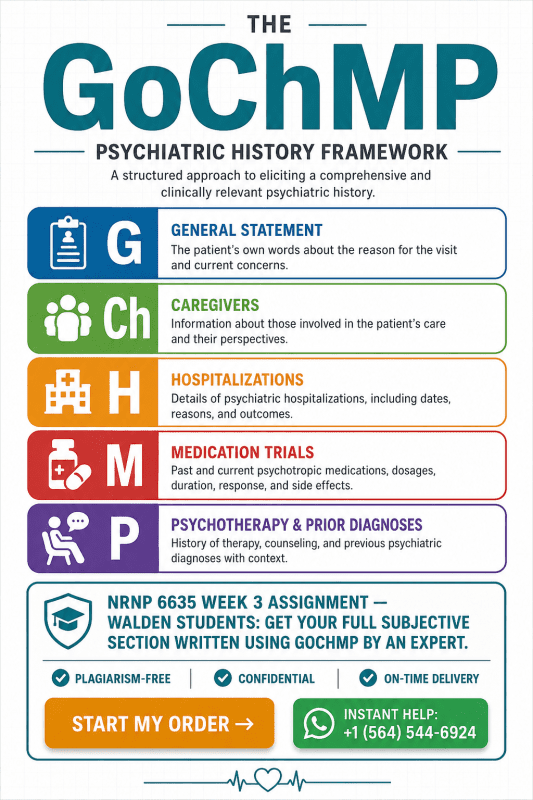
The GoChMP mnemonic organizes past psychiatric history into five domains. It is used in NRNP 6635 and appears explicitly in the Comprehensive Psychiatric Evaluation Exemplar. Every letter stands for a critical data point:
- G — General Statement: The patient’s first treatment experience. Example: “The patient entered outpatient counseling at age 16 for depressive episodes during her parents’ divorce.”
- Ch — Caregivers: List any formal caregivers involved in the patient’s psychiatric treatment, if applicable.
- H — Hospitalizations: Number of psychiatric admissions, dates, locations. Include detox episodes, residential treatment. Document any suicidal/homicidal behaviors or self-harm history.
- M — Medication Trials: List all prior psychotropics with response: Effective, Not Effective, or Adverse Reaction. This is clinically vital — a patient who experienced a hypomanic switch on sertraline has a documented flag for bipolar spectrum.
- P — Psychotherapy / Prior Diagnoses: Type of therapy, helpfulness, and all previous psychiatric diagnoses from other providers. Prior MDD diagnoses that later look like Bipolar II are extremely common.
Family Psychiatric History and Social History: The SDOH Lens
Document all first-degree relatives with psychiatric illness, substance use disorders, or suicide. First-degree family history of bipolar disorder significantly increases the pre-test probability of a bipolar diagnosis in your patient.
The social history should embed a social determinants of health (SDOH) perspective from the start — not just in the reflection. Housing stability, income, educational level, employment status, cultural background, and legal history all directly affect presentation, diagnosis, and treatment planning.
Review of Systems (ROS): Head-to-Toe with Mood Relevance
The ROS is not the physical exam — it is a system-by-system verbal survey of what the patient reports. For mood disorder evaluations, these systems carry the most diagnostic weight:
- ENDOCRINOLOGIC: Thyroid dysfunction is the most common medical mimic of both depression (hypothyroidism) and mania (hyperthyroidism). Ask about heat/cold intolerance, polyuria, polydipsia.
- NEUROLOGICAL: Headaches (lithium toxicity if already prescribed), seizure history (anticonvulsants used as mood stabilizers), cognitive changes.
- CARDIOVASCULAR: Palpitations may indicate anxiety comorbidity or stimulant/caffeine use.
- GASTROINTESTINAL: Appetite and weight changes are core mood disorder symptoms.
How to Write the Objective Section (20 Points)
The objective section documents what the clinician observes and measures. Even when no formal physical exam is conducted during a video session, you must document observable findings from the video itself and describe what the clinician should physically assess.
Physical Examination Documentation
Document findings head-to-toe for systems pertinent to the chief complaint. The exemplar is explicit: do not use “WNL” or “normal” — describe exactly what you observe. For a mood disorder evaluation, always document:
- General: Appearance, grooming, hygiene, psychomotor activity (agitation vs. retardation), level of alertness
- HEENT: Eye contact, facial expression, signs of thyromegaly on neck palpation if applicable
- Neurological: Gross motor function, gait, fine motor tremor (medication side effect screening)
- Cardiovascular: Heart rate regularity (tachycardia in anxiety/mania; bradycardia in hypothyroid depression)
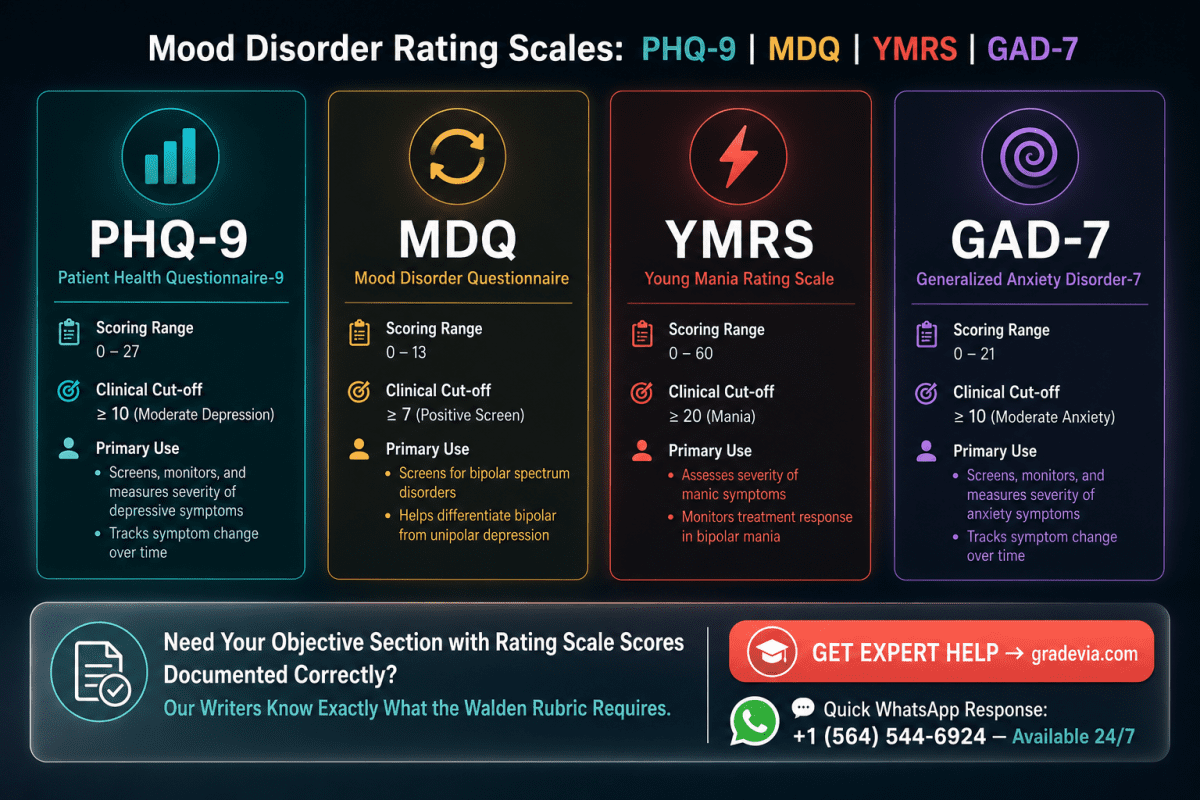
Validated Rating Scales for Mood Disorder Assessment
Rating scales are objective diagnostic tools that belong in the objective section with documented scores and clinical interpretation. Use these for mood disorder evaluations:
- PHQ-9 (Patient Health Questionnaire-9): Scores depression severity from 0–27. Score ≥10 = moderate depression; ≥20 = severe.
- MDQ (Mood Disorder Questionnaire): Screens for bipolar disorder. ≥7 of 13 items + clustering + functional impairment = positive screen; sensitivity ~73%, specificity ~90% (Hirschfeld et al., 2000, PMC314375).
- YMRS (Young Mania Rating Scale): Quantifies manic symptom severity; 11 items scored 0–4 or 0–8.
- GAD-7: Rules out Generalized Anxiety Disorder as primary diagnosis.
- PHQ-A: Adolescent version of PHQ-9; use for pediatric cases.
Recommended Laboratory Diagnostics and Rationale
Every diagnostic ordered must include an evidence-based rationale. The rubric explicitly requires this. Standard workup for a new mood disorder presentation includes:
- TSH / Free T4: Rule out hypothyroidism (mimics depression) and hyperthyroidism (mimics mania/anxiety)
- CMP: Electrolyte imbalances (hyponatremia, hypercalcemia) can cause mood symptoms; baseline for medication monitoring
- CBC: Anemia causes fatigue and cognitive slowing mimicking depression
- Urine Drug Screen: Rule out substance-induced mood disorder — required to apply DSM-5-TR mood disorder criteria
- Serum B12 / Folate: Deficiencies are associated with depressive symptoms and poor antidepressant response
- Lithium level (if prescribed): Target therapeutic range 0.6–1.2 mEq/L
How to Write the Mental Status Examination (MSE) in Paragraph Form
The mental status examination must be written as a flowing paragraph narrative, not a checklist. This is an explicit rubric requirement that students frequently miss, resulting in lost points. The MSE paragraph covers eleven domains in sequence.
The Eleven MSE Domains and Their Mood Disorder Significance
- Appearance: Grooming, hygiene, dress appropriateness. Mania: disheveled or flamboyant. Depression: neglected self-care.
- Attitude/Behavior: Cooperative, guarded, hostile, evasive. Manic patients may be expansive or irritable.
- Psychomotor Activity: Agitation (mania), retardation (depression), or mixed.
- Speech: Rate, volume, tone, fluency. Pressured speech is a hallmark of mania; slowed monotone is classic depression.
- Mood (subjective): The patient’s self-reported emotional state in their own words: “I feel wired” or “I feel empty.”
- Affect (objective): The clinician’s observed emotional expression. Assess range (broad vs. restricted/flat), congruence with mood, and stability.
- Thought Process: Goal-directed and logical vs. circumstantial, tangential, or flight of ideas (mania).
- Thought Content: Presence of SI/HI, obsessions, delusions (grandiosity in mania; nihilistic in psychotic depression).
- Perceptual Disturbances: Hallucinations (auditory/visual); pseudohallucinations; illusions.
- Cognition: Alert and oriented (person/place/time/event); recent and remote memory; concentration; abstraction.
- Insight and Judgment: Does the patient recognize they are unwell? Can they make reasonable decisions about their care?
MSE Paragraph Example: Manic Presentation
J.T. is a 28-year-old male who appears his stated age. He presents disheveled, wearing mismatched clothing, and is hyperactive throughout the interview. His speech is pressured, rapid, and loud, with frequent interruptions. He describes his mood as “fantastic — I’ve never felt better,” though his affect is labile, shifting between euphoria and irritability within minutes. His thought process is tangential with loosening of associations.
Thought content is notable for grandiose ideation; he reports he is “working on three business deals that will make me a billionaire.” He denies auditory or visual hallucinations. There is no current suicidal or homicidal ideation. Cognitively, he is alert and oriented to person, place, time, and event; however, his concentration is markedly impaired and his insight into the severity of his symptoms is poor. Judgment is compromised.
MSE Paragraph Example: Depressive Presentation
M.L. is a 42-year-old female who appears older than her stated age. She presents with poor grooming and downcast gaze, and demonstrates significant psychomotor retardation. Speech is soft, slow, and monotone, with prolonged response latency. She reports her mood as “completely empty,” and her affect is flat and constricted, congruent with her stated mood. Thought process is linear and logical, though slowed.
Thought content is notable for passive suicidal ideation without plan or intent; she denies homicidal ideation. There are no perceptual disturbances. Cognitively, she is alert and oriented x4; remote memory is intact, but recent memory and concentration are impaired. Insight is fair; judgment is mildly impaired.
How to Write Differential Diagnoses Using DSM-5-TR Criteria (25 Points)
The assessment section carries the most rubric weight at 25 points. You must list at least three differential diagnoses from highest to lowest priority, each supported by DSM-5-TR criteria, pertinent positives, and pertinent negatives. You must then explain your critical-thinking process for selecting the primary diagnosis.
What Are Pertinent Positives and Pertinent Negatives?
A pertinent positive is a symptom or finding present in the patient that supports a specific diagnosis. A pertinent negative is an expected symptom of a diagnosis that is absent — and that absence is clinically meaningful. Together, they demonstrate diagnostic rigor.
Example: For a Bipolar I diagnosis, a pertinent positive might be “three-day history of decreased need for sleep with increased energy and goal-directed activity.” A pertinent negative for MDD ruling it out might be “no prior episode of this nature; this presentation includes hypomanic features ruling out a purely unipolar course.”
Differential 1 (Primary): Bipolar I Disorder — DSM-5-TR Criteria
Bipolar I Disorder is diagnosed when there is at least one lifetime manic episode. The manic episode requires:
- Criterion A: A distinct period of abnormally elevated, expansive, or irritable mood AND persistently increased goal-directed activity or energy, lasting ≥7 days (or any duration if hospitalization required)
- Criterion B: ≥3 of 7 DIGFAST symptoms present to a significant degree (4 if mood is only irritable)
- Criterion C: Marked impairment in social/occupational functioning OR requires hospitalization OR has psychotic features
- Criterion D: Episode not attributable to substances or another medical condition
- Criterion E: Episode not better explained by schizoaffective disorder or is not superimposed on schizophrenia
The DSM-5-TR (APA, 2022) emphasizes that the addition of Criterion A’s energy/activity requirement from DSM-5 was designed to improve diagnostic specificity, particularly for Bipolar II, and to reduce overdiagnosis.
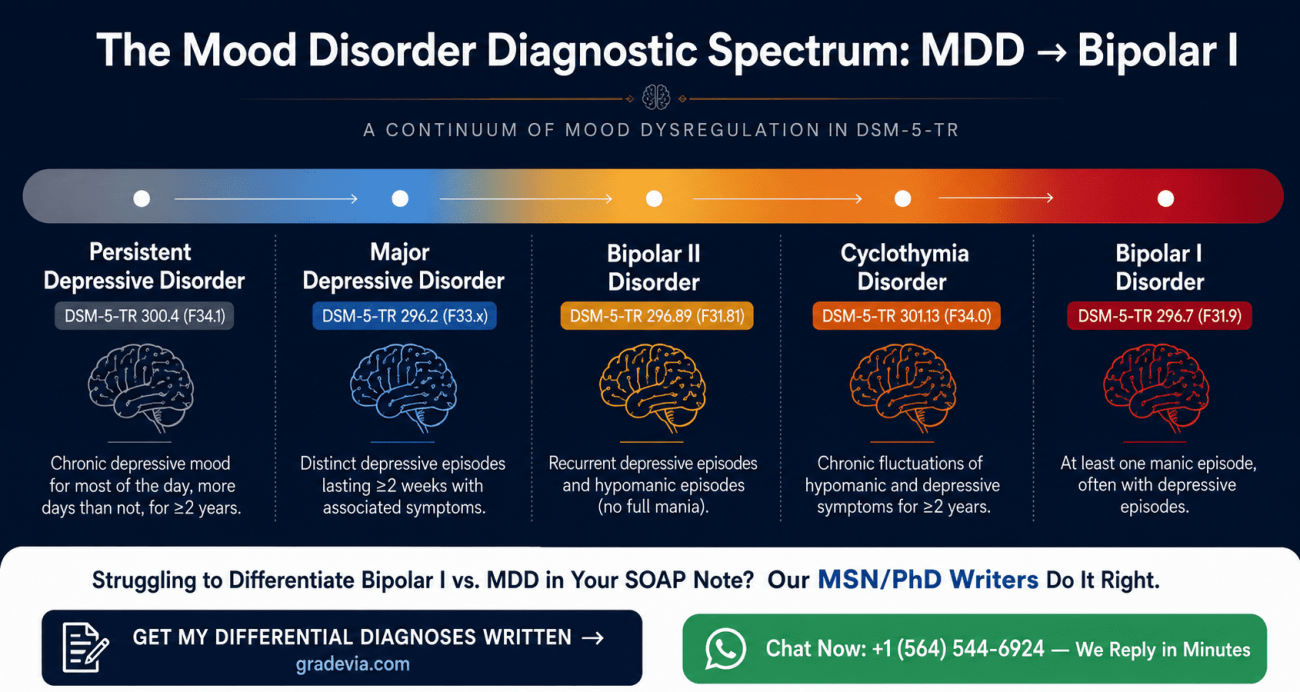
Differential 2: Major Depressive Disorder — Where MDD and Bipolar Diverge
MDD requires five or more SIGECAPS symptoms during the same 2-week period, with at least one being depressed mood or anhedonia. The critical rule-out: MDD cannot be diagnosed if there has ever been a manic or hypomanic episode. This is the most clinically consequential distinction in the mood disorder differential.
When writing your differential, document explicitly: Has this patient ever experienced a period of elevated, expansive, or irritable mood with increased energy? If the case history or video suggests any such history — even briefly or implicitly — you must address it. Missing prior manic/hypomanic history is how bipolar disorder is misdiagnosed as MDD.
Differential 3: Cyclothymic Disorder, DMDD, or Persistent Depressive Disorder
Your third differential should reflect the specific case. For adolescent patients, Disruptive Mood Dysregulation Disorder (DMDD) must be considered when the presentation involves persistent irritability and severe temper outbursts — Kaplan and Sadock (2022, Chapter 2.11) note that DMDD was added to DSM-5 specifically to prevent overdiagnosis of bipolar disorder in children.
For adult patients with chronic low-grade depression, Persistent Depressive Disorder (PDD/dysthymia) is the appropriate third differential — depressed mood for most of the day, more days than not, for at least two years, with ≥2 of six additional symptoms.
For subthreshold cycling that does not meet Bipolar I or II criteria: Cyclothymic Disorder — numerous periods of hypomanic and depressive symptoms over at least two years, never meeting full episode criteria.
How to Write Reflection Notes That Earn Full Marks (10 Points)
The reflection section is where students most commonly lose points — not because the content is hard, but because they default to superficial answers about confidentiality. The rubric explicitly instructs: “demonstrate critical thinking beyond confidentiality and consent for treatment.” Here is what that means in practice.
Legal and Ethical Considerations Beyond Confidentiality
The following legal and ethical issues are expected to be addressed in a high-scoring reflection for a mood disorder case:
- Duty to warn (Tarasoff doctrine): If a patient with mania or psychotic depression expresses homicidal ideation, the PMHNP has a legal and ethical obligation to warn identifiable third parties in applicable states.
- Involuntary psychiatric hold: Criteria for a 5150/5250 hold (or state-equivalent) — imminent danger to self or others, or gravely disabled. Mood disorder patients, especially during manic or severe depressive episodes, may meet these criteria.
- Mandated reporting: If the patient discloses child, elder, or dependent adult abuse, the PMHNP is a mandated reporter regardless of the psychiatric context.
- Medication risks and informed consent: Lithium has a narrow therapeutic index; valproate is teratogenic. These require documented, detailed informed consent beyond a standard signature.
- Cultural competence as an ethical obligation: Failing to account for cultural norms around emotional expression, help-seeking, and stigma can lead to misdiagnosis. This is both an ethical and clinical issue.
Social Determinants of Health and Health Promotion by Patient Demographics
Your reflection should tailor the SDOH discussion to your specific patient. Generic statements earn Fair marks. Specific, patient-anchored analysis earns Excellent marks.
- Adolescent patients: School-based mental health resources, parental involvement in treatment, impact of social media on mood cycling, stigma barriers in peer groups
- Military/veteran patients: VA mental health services, MST (military sexual trauma) screening, risk of underreporting mood symptoms due to career implications
- Older adult patients: Medication interactions, isolation as a mood trigger, cognitive decline mimicking depressive symptoms
- Patients from communities of color: Higher rates of misdiagnosis, mistrust of the medical system, culturally specific expressions of distress (somatization, cultural idioms)
What Would You Do Differently? Writing a Meaningful Answer
Avoid generic answers like “I would ask more questions.” Instead, anchor your reflection to a specific moment in the interview: “I would have administered the Mood Disorder Questionnaire (MDQ) before the clinical interview began, to identify bipolar screening flags before anchoring on the depressive presentation.”
Evidence-Based References: Meeting the 15-Point Criterion
You need at least three peer-reviewed sources from the last five years (2021–2026). The course required readings count toward this requirement. Always format in APA 7th edition.
Required Course Sources (APA 7th Edition Format)
- American Psychiatric Association. (2022). Bipolar and related disorders. In Diagnostic and statistical manual of mental disorders (5th ed., text rev.). https://doi.org/10.1176/appi.books.9780890425787.x03_Bipolar_and_Related_Disorders
- American Psychiatric Association. (2022). Depressive disorders. In Diagnostic and statistical manual of mental disorders (5th ed., text rev.). https://doi.org/10.1176/appi.books.9780890425787.x04_Depressive_Disorders
- Boland, R., Verduin, M. L., & Ruiz, P. (2022). Kaplan & Sadock’s synopsis of psychiatry (12th ed.). Wolters Kluwer.
High-Quality Supplemental Sources (Search These Databases)
Use PubMed, CINAHL, or PsycINFO with these search strategies:
- Bipolar vs. MDD differential: Search “differential diagnosis bipolar major depressive disorder DSM-5” — Journal of Clinical Psychiatry and Psychiatric Services publish frequently on this.
- Mental status examination: Sadock, B. J., et al. (2023) Kaplan & Sadock’s comprehensive textbook of psychiatry; or StatPearls via NCBI: Ruiz M.A. et al. “Mental Status Examination” (continuously updated).
- MDQ validity: Hirschfeld R.M.A. et al. (2000). “The Mood Disorder Questionnaire: a simple, patient-rated screening instrument for bipolar disorder.” Primary Care Companion to the Journal of Clinical Psychiatry, 2(4).
- SDOH and psychiatric diagnosis: Search “social determinants of health psychiatric evaluation” — SAMHSA guidelines and NIMH resources are current and authoritative.
NRNP 6635 Week 3 Assignment Rubric Walkthrough
Use this table as your final self-check before submission. Every Excellent-tier criterion is specific — not vague. Knowing exactly what earns top marks eliminates guesswork.
| Criterion | Points | Excellent-tier requirement |
| Subjective section | 20 pts | Thorough CC, HPI, past psychiatric history, GoChMP, substance use, social, medical history, allergies, and full ROS |
| Objective section | 20 pts | Complete physical exam documentation and diagnostics with evidence-based rationale for every test ordered |
| Assessment section | 25 pts | MSE in paragraph form; 3+ differentials with DSM-5-TR criteria comparison; pertinent positives and negatives; critical-thinking narrative |
| Reflection notes | 10 pts | Thoughtful; addresses legal/ethical issues beyond confidentiality; SDOH; health promotion by patient demographics |
| References | 15 pts | 3+ current (≤5 years), peer-reviewed articles or clinical guidelines with strong justification; APA 7th edition format |
| Written expression & formatting | 10 pts | Clear purpose statement, introduction, conclusion; smooth paragraph flow; correct grammar, spelling, punctuation throughout |
Most common point-loss patterns: (1) MSE written as a checklist instead of paragraph; (2) reflection that only addresses confidentiality; (3) differential diagnoses without DSM-5-TR criteria comparison; (4) references older than 5 years or not peer-reviewed.
Frequently Asked Questions (People Also Ask)
What is the GoChMP mnemonic in psychiatry?
GoChMP stands for General statement, Caregivers, Hospitalizations, Medication trials, and Psychotherapy/Prior diagnoses. It is used in NRNP 6635 to organize the Past Psychiatric History section of a comprehensive evaluation. Each letter prompts a specific category of information critical for building a complete psychiatric history and informing the differential diagnosis.
How do you write a mental status exam in paragraph form?
Write the MSE as a flowing narrative that covers all eleven domains in sequence: appearance, attitude/behavior, psychomotor activity, speech, mood (subjective), affect (objective), thought process, thought content, perceptual disturbances, cognition, and insight/judgment. Do not use a checklist or table format — the NRNP 6635 rubric explicitly requires paragraph form, and using a checklist results in point deductions.
What are pertinent positives and negatives in a psychiatric evaluation?
Pertinent positives are symptoms or findings present in the patient that support a specific diagnosis. Pertinent negatives are expected symptoms of a diagnosis that are absent, and their absence is clinically significant. Together they demonstrate rigorous diagnostic reasoning and are explicitly required in the NRNP 6635 Assessment section rubric.
What is the difference between Bipolar I and Bipolar II in DSM-5-TR?
Bipolar I requires at least one full manic episode (≥7 days, with marked impairment or hospitalization). Bipolar II requires at least one hypomanic episode (≥4 days, without marked impairment) and at least one major depressive episode — a full manic episode rules out Bipolar II. The distinction matters clinically because treatment protocols and prognosis differ significantly between the two.
How do I write a reflection that goes beyond confidentiality in NRNP 6635?
Address specific legal and ethical issues relevant to the case — such as duty to warn, involuntary hold criteria, mandated reporting, or teratogenic medication risks. Then discuss social determinants of health tailored to the patient’s demographics (age, ethnicity, socioeconomic status). The rubric rewards critical thinking that connects ethical obligations to the specific clinical scenario, not generic statements about HIPAA.
Author Bio
Dan Palmer, MSN
Dan Palmer is a professional psychiatric mental health writer with 14 years of writing practice experience in psychiatric mental health topics. He has written about various topics covering Walden University nursing courses like NRNP 6635 Psychopathology and Diagnostic Reasoning and other related graduate courses. His scholarly interests include depression screening in medically complex patients, culturally responsive psychiatric assessment, and standardized rating scale optimization in primary care psychiatry. Connect with him: https://www.linkedin.com/in/dan-palmer-a49378108
Originally written on June 1, 2026