Assessing and Diagnosing Patients With Mood Disorders Sample: NRNP/PRAC 6635 Week 3

Assessing and Diagnosing Patients With Mood Disorders Sample: NRNP/PRAC 6635 Week 3
Assignment
Accurately diagnosing depressive disorders can be challenging given their periodic and, at times, cyclic nature. Some of these disorders occur in response to stressors and, depending on the cultural history of the client, may affect their decision to seek treatment. Bipolar disorders can also be difficult to properly diagnose. While clients with a bipolar or related disorder will likely have to contend with the disorder indefinitely, many find that the use of medication and evidence-based treatments have favorable outcomes.
Resources
Be sure to review the Learning Resources before completing this activity.
Click the weekly resources link to access the resources.
To Prepare:
- Review this week’s Learning Resources. Consider the insights they provide about assessing and diagnosing mood disorders.
- Download the Comprehensive Psychiatric Evaluation Template, which you will use to complete this Assignment. Also review the Comprehensive Psychiatric Evaluation Exemplar to see an example of a completed evaluation document.
- By Day 1 of this week, select a specific video case study to use for this Assignment from the Video Case Selections choices in the Learning Resources. View your assigned video case and review the additional data for the case in the “Case History Reports” document, keeping the requirements of the evaluation template in mind.
- Consider what history would be necessary to collect from this patient.
- Consider what interview questions you would need to ask this patient.
- Identify at least three possible differential diagnoses for the patient.
By Day 7 of Week 3
Complete and submit your Comprehensive Psychiatric Evaluation, including your differential diagnosis and critical-thinking process to formulate a primary diagnosis. Incorporate the following into your responses in the template:
- Subjective: What details did the patient provide regarding their chief complaint and symptomology to derive your differential diagnosis? What is the duration and severity of their symptoms? How are their symptoms impacting their functioning in life?
- Objective: What observations did you make during the psychiatric assessment?
- Assessment: Discuss the patient’s mental status examination results. What were your differential diagnoses? Provide a minimum of three possible diagnoses with supporting evidence, listed in order from highest priority to lowest priority. Compare the DSM-5-TR diagnostic criteria for each differential diagnosis and explain what DSM-5 criteria rules out the differential diagnosis to find an accurate diagnosis. Explain the critical-thinking process that led you to the primary diagnosis you selected. Include pertinent positives and pertinent negatives for the specific patient case.
Reflection notes: What would you do differently with this client if you could conduct the session over? Also include in your reflection a discussion related to legal/ethical considerations (demonstrate critical thinking beyond confidentiality and consent for treatment!), health promotion and disease prevention taking into consideration patient factors (such as age, ethnic group, etc.), PMH, and other risk factors (e.g., socioeconomic, cultural background, etc.).
Assessing and Diagnosing Patients With Mood Disorders Sample: Week 3: Training Title 2
Subjective:
CC (chief complaint): “I just feel really sad and I don’t know why. I can’t focus in school and I don’t really feel like doing anything anymore.”
HPI: N.C. is a 17-year-old African American female who presents for an initial psychiatric evaluation referred by her dormitory resident advisor following observed behavioral and mood changes over the past six to eight weeks. She is not currently prescribed any psychotropic medications. She relocated from New Orleans, Louisiana to Chicago, Illinois to enroll in an accelerated high school business program and now resides in a campus dormitory, away from her family for the first time.
N.C. reports a persistently depressed mood that she describes as feeling “empty and heavy” most of the day, nearly every day since arriving at school. She endorses anhedonia, stating she no longer enjoys activities she previously found pleasurable, including socializing and listening to music.
She reports significant difficulty concentrating on coursework, describing her mind as “going blank” during class, which is particularly distressing given the academic demands of her accelerated program. She endorses fatigue and low energy, noting she often sleeps 10–11 hours yet wakes feeling unrefreshed. She reports a weight gain of approximately eight pounds since the relocation, consistent with increased appetite specifically for carbohydrate-heavy comfort foods. She denies early morning awakening but endorses hypersomnia.
She endorses feelings of worthlessness and guilt, expressing self-blame for what she perceives as academic failure despite maintaining passing grades. She denies active suicidal ideation, plan, or intent at this time; however, she reports passive death ideation, stating, “Sometimes I think everyone would be better off without me.”
This statement requires close monitoring. She denies homicidal ideation, auditory or visual hallucinations, paranoia, grandiosity, or manic or hypomanic episodes. She denies periods of elevated or expansive mood, decreased need for sleep, impulsivity, or increased goal-directed behavior.
Symptom onset correlates directly with her relocation and enrollment approximately eight weeks ago. Prior to this move, she describes her mood as “normal” and her functioning as high. Symptom severity is moderate to moderately severe by clinical impression, with functional impairment across academic performance, social engagement, and self-care. She works part-time at a local coffee shop and reports difficulty maintaining reliability in her shift attendance over the past three weeks.
Past Psychiatric History:
General Statement: No prior psychiatric treatment. N.C. has no known history of outpatient therapy, inpatient psychiatric hospitalization, or psychotropic medication use prior to this evaluation.
Caregivers: Not applicable. Patient is 17 years old and resides independently in a supervised dormitory. Parents are biological and remain in New Orleans, Louisiana.
Hospitalizations: None. No inpatient psychiatric admissions, no emergency psychiatric evaluations, no detox or residential treatment history.
Medication Trials: None. No prior psychotropic medication trials.
Psychotherapy or Previous Psychiatric Diagnosis: None reported. N.C. denies any formal psychiatric diagnosis. Family history is notable for depression (see Family History), but no formal diagnosis has been assigned to the patient previously.
Substance Current Use and History: N.C. denies any current or historical use of alcohol, cannabis, tobacco, or illicit substances. She denies any substance use history within the family unit, which is consistent with case history documentation.
Family Psychiatric/Substance Use History: Family history is positive for depression on at least one side of the family, per case history. No family history of bipolar disorder, psychosis, or completed suicide is reported. No family substance use history documented.
Psychosocial History: N.C. was born and raised in New Orleans, Louisiana, where she lived with both biological parents and four brothers. She describes her pre-relocation life as socially rich and family-centered. She currently lives in an on-campus dormitory for her accelerated high school business program in Chicago, Illinois—her first extended separation from her family. She is not in a romantic relationship and identifies as heterosexual.
She is a full-time student and works part-time at a local coffee shop. She has no legal history. She denies any history of physical, sexual, or emotional abuse. She reports feeling isolated and disconnected from her new environment, describing difficulty forming peer connections in the dormitory. She identifies the abrupt change in her social support network as a significant stressor. She endorses academic pressure as a compounding factor.
Medical History: No known medical illnesses. No history of seizures, head trauma, thyroid disease, diabetes, or neurological disorders. No surgeries reported.
Current Medications: None.
Allergies: NKDA. No known food or environmental allergies reported.
Reproductive Hx: LMP reported as regular and occurring within the past month. Not pregnant. Not nursing. Denies contraceptive use. Denies sexual activity at this time. No sexual concerns voiced.
ROS:
GENERAL: Endorses fatigue, hypersomnia (10–11 hours/night), and weight gain of approximately 8 lbs. over the past 8 weeks. Denies fever, chills, or diaphoresis.
HEENT: Denies headache, visual changes, blurred or double vision, yellow sclerae, hearing difficulty, nasal congestion, sore throat, or dental pain.
SKIN: Denies rash, lesions, pruritus, or abnormal skin changes.
CARDIOVASCULAR: Denies chest pain, palpitations, chest pressure, or lower extremity edema.
RESPIRATORY: Denies dyspnea, cough, wheezing, or sputum production.
GASTROINTESTINAL: Endorses increased appetite with preference for carbohydrate-heavy foods. Denies nausea, vomiting, diarrhea, constipation, or abdominal pain.
GENITOURINARY: Denies dysuria, urinary urgency, frequency, or abnormal discharge.
NEUROLOGICAL: Endorses subjective difficulty with concentration. Denies headache, dizziness, syncope, numbness, tingling, or motor deficits.
MUSCULOSKELETAL: Denies muscle or joint pain, stiffness, or limited range of motion.
HEMATOLOGIC: Denies anemia, easy bruising, or abnormal bleeding.
LYMPHATICS: Denies lymphadenopathy or history of splenectomy.
ENDOCRINOLOGIC: Denies heat or cold intolerance, polyuria, polydipsia, or excessive sweating. Thyroid pathology not previously diagnosed; thyroid function labs warranted given mood and weight changes.
Objective:
Physical Exam: N.C. is a 17-year-old African American female who appears her stated age. Vital signs: T 97.4°F, P 82 bpm, R 20 breaths/min, BP 128/84 mmHg, Ht 5’2″, Wt 192 lbs (BMI ~35.1, indicating obesity class I, clinically relevant to differential workup). General: Alert, oriented, appears tired. Mildly disheveled but adequately dressed for the weather. HEENT: Normocephalic, atraumatic. Sclerae clear, no icterus. Oropharynx clear. Cardiovascular: Regular rate and rhythm, no murmurs. Respiratory: Clear to auscultation bilaterally. Neurological: Cranial nerves II–XII grossly intact. Gait steady. No focal neurological deficits.
Diagnostic Results: No recent labs on file. The following are clinically indicated to rule out organic contributors to depressive symptomatology:
CBC with differential – to rule out anemia as contributor to fatigue and low energy
CMP – baseline metabolic panel given weight and appetite changes
TSH with reflex free T4 – hypothyroidism presents with hypersomnia, weight gain, fatigue, and dysphoria, directly overlapping with current presentation
Urine toxicology screen – baseline; patient denies substance use but screening is standard prior to initiating pharmacotherapy
Vitamin D and B12 levels – deficiencies in adolescent females are associated with depressive symptoms and fatigue
Urine pregnancy test – standard protocol for adolescent females prior to any pharmacotherapy initiation
Assessment:
Mental Status Examination: N.C. is a 17-year-old African American female who appears her stated age. She presents to the interview accompanied by her dormitory resident advisor. She is cooperative throughout the assessment, though she makes limited spontaneous eye contact and requires gentle encouragement to elaborate on her responses. She is adequately groomed but appears mildly fatigued, with slightly disheveled clothing.
No abnormal motor activity, psychomotor agitation, or psychomotor retardation is observed. Speech is soft in volume, slow in rate, and low in spontaneity; she speaks only when directly questioned. Tone is monotone. Thought process is linear, logical, and goal-directed without loosening of associations or tangentiality. Thought content is significant for passive suicidal ideation (“Sometimes I think everyone would be better off without me”) without active intent, plan, or means; no homicidal ideation is present.
She denies auditory hallucinations, visual hallucinations, and there is no evidence of perceptual disturbance during the interview. No delusional content elicited. Mood is self-described as “sad and empty.” Affect is dysphoric, restricted in range, and congruent with reported mood. No evidence of hypomanic or manic features. Cognitively, she is alert and oriented to person, place, time, and situation (A&Ox4).
Recent and remote memory appear grossly intact. She demonstrates mildly impaired concentration during the interview, requiring occasional repetition of questions. Insight is fair; she recognizes that her mood has changed but minimizes the severity. Judgment is fair; she agreed to this evaluation at the recommendation of her resident advisor.
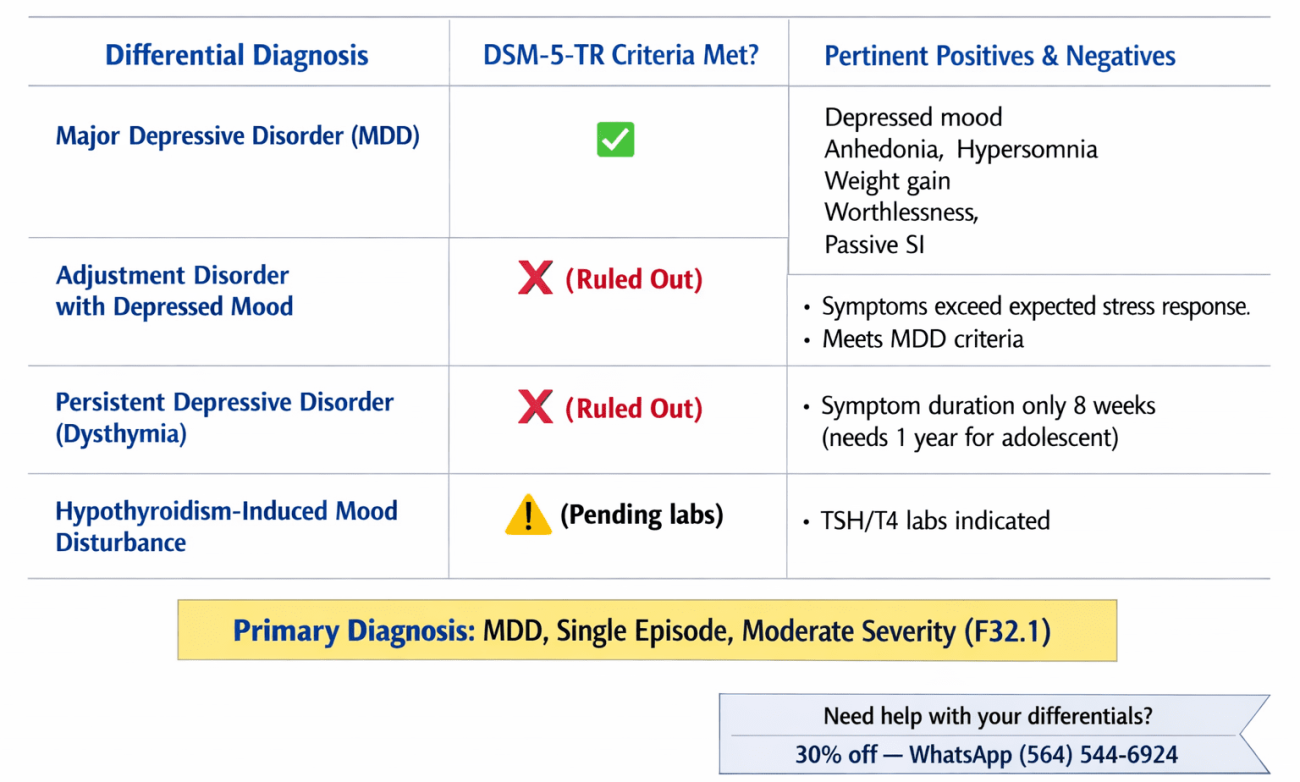
Differential Diagnoses:
1. Major Depressive Disorder (MDD), Single Episode, Moderate Severity (Primary Diagnosis) — F32.1
MDD is the primary diagnostic impression for N.C. Per DSM-5-TR criteria (American Psychiatric Association [APA], 2022), a diagnosis of MDD requires five or more of the following symptoms during a two-week period, with at least one being depressed mood or anhedonia: (1) depressed mood most of the day, nearly every day; (2) markedly diminished interest or pleasure in all or most activities; (3) significant weight change or appetite disturbance; (4) insomnia or hypersomnia; (5) psychomotor agitation or retardation; (6) fatigue or loss of energy; (7) feelings of worthlessness or excessive guilt; (8) diminished ability to think or concentrate; and (9) recurrent thoughts of death or suicidal ideation.
Pertinent positives for N.C.: persistently depressed mood (criterion 1), anhedonia—loss of interest in previously enjoyed activities including socialization and music (criterion 2), hyperphagia with weight gain (criterion 3), hypersomnia with non-restorative sleep (criterion 4), fatigue and low energy (criterion 6), worthlessness and self-blame (criterion 7), concentration difficulty affecting academic performance (criterion 8), and passive suicidal ideation (criterion 9).
This constitutes at least seven of nine required criteria, with both anchor symptoms present (depressed mood and anhedonia), meeting threshold for a diagnosis of moderate severity. Symptom duration is eight weeks, well exceeding the minimum two-week threshold. Functional impairment is documented across academic, occupational, and social domains.
Pertinent negatives: No manic or hypomanic episodes, no psychotic features, no identified general medical condition currently confirmed to account for symptoms (hypothyroidism pending workup), no bereavement-only context, no substance use contributing to presentation.
2. Adjustment Disorder with Depressed Mood (Rule Out) — F43.21
Adjustment Disorder with Depressed Mood is a plausible differential given the clear temporal relationship between N.C.’s relocation to Chicago and symptom onset (APA, 2022). DSM-5-TR criteria require emotional or behavioral symptoms in response to an identifiable stressor, occurring within three months of stressor onset, with clinically significant distress or functional impairment disproportionate to the severity or intensity of the stressor. The relocating to a competitive academic environment away from all family and social support represents a significant psychosocial stressor, and this differential must be considered.
However, adjustment disorder is ruled out as the primary diagnosis because the breadth, number, and severity of N.C.’s symptoms exceed what would be expected in an adjustment disorder presentation. Specifically, N.C. meets criteria for at least seven of nine MDD symptoms, including passive suicidal ideation, anhedonia, hypersomnia, and worthlessness—symptoms that go beyond the low-grade mood disturbance characteristic of adjustment disorder.
Furthermore, DSM-5-TR specifies that adjustment disorder is not diagnosed when criteria for another specific disorder are met. Because N.C. meets full criteria for MDD, adjustment disorder is superseded as the more accurate diagnosis.
3. Persistent Depressive Disorder (Dysthymia) (Rule Out) — F34.1
Persistent Depressive Disorder (PDD) requires a depressed mood for most of the day, for more days than not, for at least two years in adults (one year in children and adolescents), with at least two associated symptoms (APA, 2022). Given that N.C. is 17 years old, the one-year threshold applies. This differential is considered because the case history documents a family history of depression, and early-onset, lower-grade chronic depression is relevant to this demographic.
PDD is ruled out as the primary diagnosis based on chronology: N.C.’s symptoms have been present for approximately eight weeks, which does not meet the required one-year minimum in adolescents. Additionally, her prior functioning was described as high and mood as normal prior to relocation, which contradicts the persistent, chronic nature required for a PDD diagnosis.
However, if symptoms persist beyond the one-year threshold or do not fully remit with treatment, reassessment for PDD or a “double depression” presentation (MDD superimposed on PDD) would be warranted longitudinally.
4. Hypothyroidism-Induced Mood Disturbance (Rule Out) — E03.9
Hypothyroidism shares significant phenotypic overlap with MDD, including fatigue, hypersomnia, weight gain, psychomotor slowing, and depressed mood (Bauer et al., 2020). N.C.’s BMI of 35.1, hypersomnia, weight gain of 8 lbs in 8 weeks, and fatigue all warrant thyroid function testing (TSH with reflex free T4) prior to initiating psychotropic medications.
A diagnosis of mood disorder due to another medical condition (hypothyroidism) would be more appropriate if labs return consistent with thyroid dysfunction. Pending these results, MDD remains the primary diagnostic impression, but pharmacotherapy initiation should be deferred until thyroid function is assessed.
Reflections:
This case presented a clinically rich example of how major life transitions—even ostensibly positive ones such as enrollment in a competitive academic program—can precipitate clinically significant depressive episodes in adolescents. N.C.’s presentation underscores that the absence of prior psychiatric history does not confer immunity to mood disorders; in fact, first-episode MDD in adolescence often emerges in the context of psychosocial stressors that disrupt established attachment and support networks (Avenevoli et al., 2015).
One area I would approach differently in a follow-up session is a more structured assessment of passive suicidal ideation using a validated tool such as the Columbia Suicide Severity Rating Scale (C-SSRS). While N.C. denied active intent or plan, passive ideation in an isolated adolescent living away from family represents a clinically serious signal that warrants ongoing, formal monitoring at every contact.
Legal and Ethical Considerations:
N.C. is a 17-year-old minor, which raises important ethical and legal dimensions. In Illinois (where she currently resides), minors may consent to certain mental health services independently; however, engaging her parents—who are in New Orleans—requires a careful balance of confidentiality, minor consent laws, and duty to warn. Given her passive suicidal ideation, a safety assessment must be completed at every session, and parents must be notified if risk escalates to active ideation with plan or intent.
The treating clinician must be familiar with Illinois minor consent statutes (410 ILCS 210) and document the rationale for any decision regarding parental notification. Additionally, as a minor working part-time while enrolled in an intensive academic program, her workplace and school should not be contacted without a properly executed release of information consistent with HIPAA and FERPA protections.
The dormitory context adds another layer: the clinician has a responsibility to ensure N.C.’s safety within a supervised residential environment and to coordinate care communication with the resident advisor in a manner that preserves her privacy to the maximum extent possible.
Health Promotion and Social Determinants of Health:
N.C. is a young African American adolescent who has been uprooted from a close-knit, family-centered environment in New Orleans and placed in a predominantly unfamiliar academic and social context in Chicago. Race and ethnicity are important contextual factors: African American adolescents with depression are statistically less likely to receive timely diagnoses and evidence-based treatment due to structural barriers including provider bias, underrepresentation in mental health settings, and culturally influenced stigma around help-seeking (Alegría et al., 2019).
The clinician must approach this case with cultural humility, recognizing that N.C.’s presentation may be filtered through a lens of stoicism or self-sufficiency that is normative in her family and cultural context.
Her academic environment represents both a stressor and a protective factor: a high-achieving peer environment can exacerbate feelings of inadequacy, but structured routine and intellectual engagement are also therapeutic when properly supported. Health promotion should emphasize sleep hygiene education, nutritional counseling to address hyperphagia, physical activity as an adjunctive mood intervention, and psychoeducation for N.C. and her parents.
Facilitating a connection with campus support services, a school counselor, or culturally affirming peer support groups would address the social isolation that is a key driver of her current presentation.
Regarding disease prevention: given the family history of depression, N.C. is at elevated genetic and environmental risk for recurrent mood episodes. Initiating evidence-based psychotherapy (cognitive behavioral therapy [CBT] is first-line for adolescent MDD) and closely monitoring whether pharmacotherapy is indicated—particularly if labs rule out hypothyroidism and symptoms fail to respond to therapy alone—represents a proactive prevention strategy for chronicity.
References
Alegría, M., Alvarez, K., Cheng, M., & Falgas-Bague, I. (2019). Recent advances on social determinants of mental health: Looking fast forward. American Journal of Psychiatry, 180(7), 473–482. https://doi.org/10.1176/appi.ajp.2023.22090955
American Psychiatric Association. (2022). Diagnostic and statistical manual of mental disorders (5th ed., text rev.). https://doi.org/10.1176/appi.books.9780890425787
Avenevoli, S., Swendsen, J., He, J. P., Burstein, M., & Merikangas, K. R. (2015). Major depression in the National Comorbidity Survey–Adolescent Supplement: Prevalence, correlates, and treatment. Journal of the American Academy of Child & Adolescent Psychiatry, 54(1), 37–44. https://doi.org/10.1016/j.jaac.2014.10.010
Bauer, M., Goetz, T., Glenn, T., & Whybrow, P. C. (2020). The thyroid-brain interaction in thyroid disorders and mood dysregulation. Journal of Neuroendocrinology, 20(10), 1101–1114. https://doi.org/10.1111/j.1365-2826.2008.01774.x
Thapar, A., Collishaw, S., Pine, D. S., & Thapar, A. K. (2012). Depression in adolescence. The Lancet, 379(9820), 1056–1067. https://doi.org/10.1016/S0140-6736(11)60871-4
Frequently Asked Questions
1. What are mood disorders?
Mood disorders are mental health conditions that primarily affect a person’s emotional state and ability to regulate mood. They cause persistent periods of depression, mania, or mood instability that interfere with daily functioning, relationships, work, and overall quality of life. Common examples include major depressive disorder, bipolar disorder, and persistent depressive disorder.
2. What is the difference between depression and bipolar disorder?
Depression involves episodes of low mood only, while bipolar disorder includes both depressive episodes and periods of mania or hypomania. People with bipolar disorder may experience extreme mood swings, increased energy, reduced need for sleep, and impulsive behavior during manic phases, followed by episodes of depression. Accurate diagnosis is important because treatment approaches differ.
3. What are the common symptoms of a mood disorder?
Common symptoms of mood disorders include persistent sadness, loss of interest in activities, changes in sleep, fatigue, and difficulty concentrating. Depending on the specific disorder, symptoms may also include elevated mood, excessive energy, irritability, racing thoughts, feelings of worthlessness, or suicidal thoughts. The severity and duration of symptoms vary among individuals.
4. What causes mood disorders?
Mood disorders are caused by a combination of genetic, biological, psychological, and environmental factors. Family history, brain chemistry imbalances, chronic stress, trauma, medical conditions, and significant life changes can all contribute to the development of a mood disorder. In most cases, no single factor is responsible.
5. Can mood disorders be treated?
Yes, mood disorders can be effectively treated with a combination of therapy, medication, and lifestyle interventions. Treatment plans often include psychotherapy, antidepressants, mood stabilizers, stress management strategies, regular exercise, and ongoing support from healthcare professionals. Early diagnosis and treatment generally lead to better outcomes.
Can this sample paper be used as a reference or guide for completing the NRNP 6635 Week 3 mood disorders assignment?
Absolutely!
Does this sample meet Walden’s updated rubric requirements for NRNP 6635 Week 3?”
Yes. This sample was written to align with the current NRNP/PRAC 6635 Week 3 rubric, covering all required sections: Subjective, Objective, MSE, three differential diagnoses with DSM-5-TR criteria, pertinent positives/negatives, and a full reflection including legal/ethical and health promotion considerations. That said, rubrics can vary by term; always cross-check with your specific rubric before submitting.
Can I use this sample as a template for my own Week 3 assignment, or will it flag for plagiarism?
Yes, you can use this sample as a reference and structural guide, but do not copy it directly; submitting it as your own will flag for plagiarism. The sample is here to show you the expected format, depth, and clinical reasoning Walden requires. If you need a completely original evaluation written for your specific case, we can handle that from scratch.
What should the reflection section of the NRNP 6635 Week 3 mood disorders assignment include beyond confidentiality?
A strong reflection section should address: (1) legal/ethical nuances specific to the patient’s context (e.g., minor consent laws, Illinois 410 ILCS 210 statutes if the patient is an adolescent, HIPAA vs. FERPA intersections in school settings); (2) a validated suicide risk tool such as the Columbia Suicide Severity Rating Scale (C-SSRS) if passive ideation is present; (3) health promotion tailored to patient demographics — sleep hygiene, nutritional counseling, culturally affirming community resources; (4) social determinants of health including race, isolation, academic pressure, and socioeconomic factors; and (5) disease prevention given family psychiatric history, with a longitudinal plan for monitoring for chronicity or recurrence.