NRNP 6635 Week 4 Comprehensive Psychiatric Evaluation Help

NRNP 6635 Week 4 Comprehensive Psychiatric Evaluation: Assessing and Diagnosing Patients With Anxiety Disorders, PTSD, and OCD
Complete and submit your Comprehensive Psychiatric Evaluation, including your differential diagnosis and critical-thinking process to formulate primary diagnosis.
Incorporate the following into your responses in the template:
- Subjective: What details did the patient provide regarding their chief complaint and symptomology to derive your differential diagnosis? What is the duration and severity of their symptoms? How are their symptoms impacting their functioning in life?
- Objective: What observations did you make during the psychiatric assessment?
- Assessment: Discuss the patient’s mental status examination results. What were your differential diagnoses? Provide a minimum of three possible diagnoses with supporting evidence, listed in order from highest priority to lowest priority. Compare the DSM-5-TR diagnostic criteria for each differential diagnosis and explain what DSM-5-TR criteria rules out the differential diagnosis to find an accurate diagnosis. Explain the critical-thinking process that led you to the primary diagnosis you selected. Include pertinent positives and pertinent negatives for the specific patient case.
- Reflection notes: What would you do differently with this client if you could conduct the session over? Also include in your reflection a discussion related to legal/ethical considerations (demonstrate critical thinking beyond confidentiality and consent for treatment!), health promotion and disease prevention taking into consideration patient factors (such as age, ethnic group, etc.), PMH, and other risk factors (e.g., socioeconomic, cultural background, etc.).
NRNP 6635 Case History Reports rev 4.26.2022-3
NRNP _PRAC_6635_ComprehensivePsychiatricEvaluationExemplar_ rev.4.2022
NRNP PRAC 6635 Comprehensive Psychiatric Evaluation Template
What This Assignment Requires
The NRNP 6635 Week 4 assignment asks Walden University PMHNP students to complete a Comprehensive Psychiatric Evaluation using the provided template, selecting one of the Week 4 video case studies involving anxiety disorders, PTSD, or OCD. You must document a full SOAP-structured evaluation; including chief complaint, HPI, GoChaMp psychiatric history, full 12-system ROS, physical exam, validated rating scales, mental status examination in paragraph form, and at least three DSM-5-TR–justified differential diagnoses. The assignment is worth 100 points and is graded on rubric criteria spanning subjective documentation, objective findings, assessment quality, reflection depth, evidence-based references, and written expression. Mastering the structure is the single fastest path to a perfect score.
What Is the NRNP 6635 Week 4 Assignment?
The NRNP 6635 Week 4 assignment is a comprehensive psychiatric evaluation focused on anxiety disorders, PTSD, and OCD. It is part of the Psychopathology and Diagnostic Reasoning course (NRNP/PRAC 6635) at Walden University’s College of Nursing, designed for students pursuing the Psychiatric-Mental Health Nurse Practitioner (PMHNP) certification.
Students select one of several video case studies from the Symptom Media library, including Training Titles 15, 21, 37, 40, 55, 85, and 95, and complete the Comprehensive Psychiatric Evaluation Template using data from both the video and the corresponding Case History Reports document. The completed evaluation must demonstrate graduate-level clinical reasoning, DSM-5-TR diagnostic competence, and scholarly APA 7th edition writing.
This is not a simple summary exercise. The rubric rewards thorough, accurate, and clinically reasoned documentation; the kind of note a PMHNP preceptor would sign off on in a real outpatient psychiatric setting.
Why Training Title 37 Is the Strongest Case Choice
Training Title 37 — featuring Mr. Luca Esposito, a 21-year-old Caucasian male from Orlando, Florida — offers the most clinically rich presentation for demonstrating diagnostic reasoning in panic disorder.
The case presents with two spontaneous panic attacks within 48 hours, an ER visit, developing anticipatory anxiety, and avoidance behaviors. These features map cleanly onto DSM-5-TR Panic Disorder criteria (F41.0) while also generating robust differential material for Generalized Anxiety Disorder (GAD), Social Anxiety Disorder, and medical causes of tachycardia. The case history also provides specific vitals, including a heart rate of 112 bpm, which adds objective clinical data.
Compared to Training Title 15 (Ralph Newsome), which is the most widely published case online and therefore the most recognizable to evaluators, Training Title 37 allows a more original, detailed evaluation while still following the same template structure. Originality in content, not format, is what distinguishes the highest-scoring submissions.
How to Write the Subjective Section for a Perfect Score
The Subjective section earns up to 20 points and must thoroughly and accurately document all required components: chief complaint, HPI, GoChaMp psychiatric history, substance use, family history, psychosocial history, medical history, current medications, allergies, reproductive history, and a full 12-system ROS.
Chief Complaint
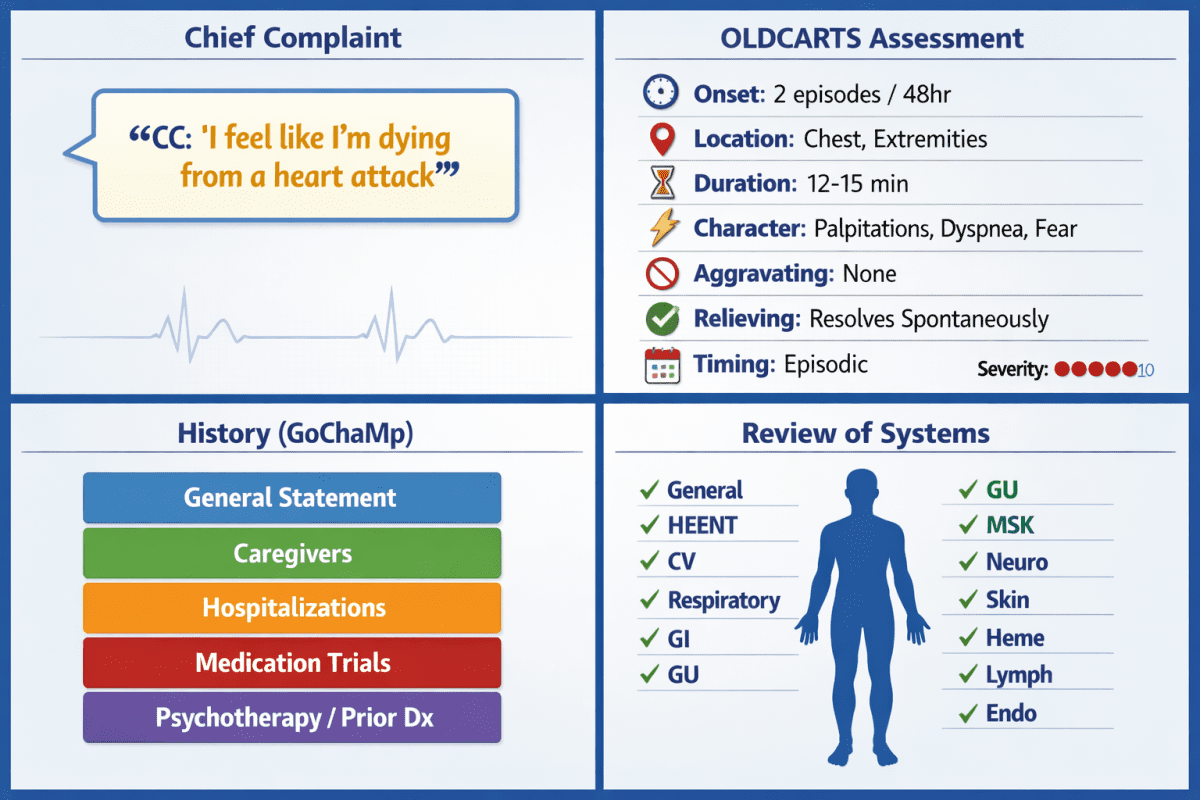
The chief complaint (CC) must be verbatim from the patient. For L.E. (Training Title 37), the CC is:
“I feel like I’m dying from a heart attack.”
This is not your paraphrase; it is the patient’s own words in quotation marks. This is a frequent error in lower-scoring submissions.
How to Write the HPI Using OLDCARTS
The HPI opens with a structured identifier sentence, then expands using symptom analysis. Begin as follows:
L.E. is a 21-year-old Caucasian male presenting for initial psychiatric evaluation for recurrent episodes of acute terror. He is not currently prescribed psychotropic medications and is self-referred following an emergency department visit.
Then document the symptom profile using OLDCARTS:
- Onset: Two episodes in two days — first while watching television, second while making coffee
- Location: Diffuse — chest, extremities, whole-body sensation
- Duration: 12 to 15 minutes per episode, self-resolving
- Character: Palpitations, diaphoresis, dyspnea, chest pain, paresthesias, dizziness, derealization, fear of dying
- Aggravating factors: No identifiable trigger; spontaneous and unexpected
- Relieving factors: Episodes resolve without intervention; patient reports attempting to stay still
- Timing: Episodic, not persistent
- Severity: Patient rates fear during episodes at 9/10
Document functional impact explicitly: L.E. has reduced his Uber driving shifts and avoids leaving his apartment alone; this is the behavioral change that supports the Panic Disorder diagnosis under DSM-5-TR Criterion B.
The GoChaMp Mnemonic for Past Psychiatric History
The GoChaMp mnemonic structures past psychiatric history across five components:
- General Statement: First treatment experience or entry point into psychiatric care. For L.E.: no prior psychiatric treatment; this is his first evaluation.
- Cha — Caregivers: Not applicable for an adult patient seen individually.
- Hospitalizations: One ER visit one week ago; not admitted. No prior inpatient psychiatric history. No detox or residential history. No suicidal or homicidal behavior history. No self-harm history.
- Medication trials: None. No prior psychotropic medication exposure.
- Psychotherapy or Prior Psychiatric Diagnosis: None reported; no prior formal psychiatric diagnosis.
This mnemonic is embedded in the Comprehensive Psychiatric Evaluation Exemplar and reflects standard documentation in psychiatric SOAP notes. Using it consistently signals clinical competence to evaluators.
Substance Use History
Document all substances — including caffeine, which is clinically relevant for panic disorder because caffeine is a methylxanthine that increases sympathetic nervous system arousal and can precipitate or exacerbate panic attacks. For L.E.: no alcohol, no illicit substances, no tobacco. Caffeine use should be asked about and documented.
Psychosocial History
Include at minimum:
- Born and raised in Buffalo, New York; currently living alone in Orlando, Florida
- Only child
- Currently single; has a long-distance girlfriend from high school
- Full-time student pursuing a graphic design degree
- Works part-time as an Uber driver
- No legal history
- No disclosed trauma history
- Routine-oriented; sleeps 6 hours per night; eats three meals daily
Full Review of Systems (ROS): All 12 Systems Required
The ROS is different from the physical exam — it documents what the patient reports, not what you observe. List all 12 systems head-to-toe with explicit positives and negatives:
- General: No weight loss, fever, chills, or fatigue
- HEENT: No visual changes, no hearing loss, no congestion
- Skin: Mild diaphoresis during episodes (positive); no rash or itching at baseline
- Cardiovascular: Palpitations (positive), chest tightness during episodes (positive), no edema
- Respiratory: Shortness of breath during episodes (positive); no chronic cough
- Gastrointestinal: Nausea reported during episodes (positive); no vomiting, diarrhea, or abdominal pain at baseline
- Genitourinary: No dysuria, urgency, or hesitancy
- Neurological: Dizziness (positive), paresthesias in extremities during episodes (positive); no syncope, seizures, or focal deficits
- Musculoskeletal: No joint pain, muscle stiffness, or back pain
- Hematologic: No anemia, bleeding, or bruising
- Lymphatics: No enlarged nodes; no splenectomy history
- Endocrinologic: No heat or cold intolerance, no polyuria or polydipsia
Failing to document all 12 systems is one of the most common reasons students lose points in the Subjective section. Most online examples omit Hematologic, Lymphatics, and Endocrinologic — which are essential for ruling out medical differentials.
How to Write the Objective Section for Full Credit
The Objective section earns up to 20 points and requires pertinent physical exam documentation, diagnostic lab rationale, and — critically — validated psychiatric rating scales.
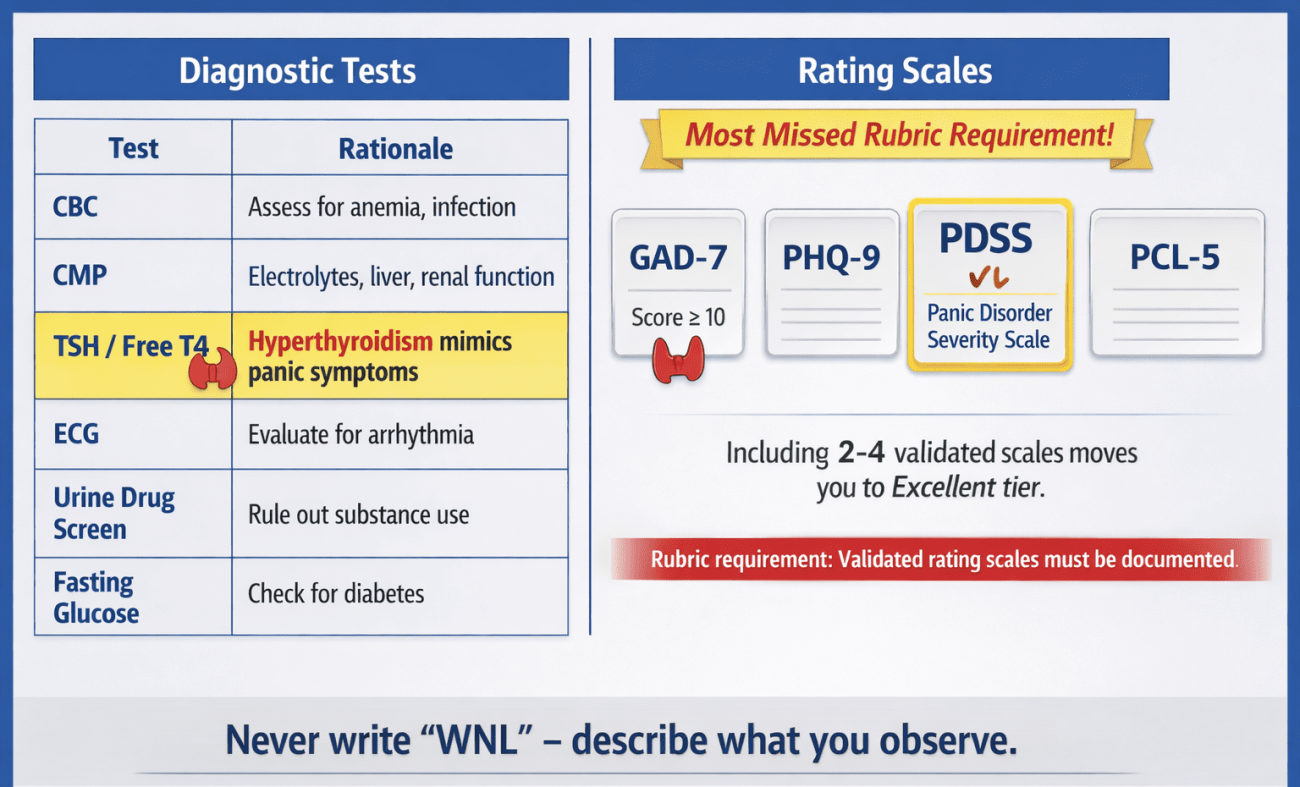
Physical Exam: Never Write “WNL”
The rubric is explicit: do not use “WNL” or “normal.” Describe what you observe. For L.E., document pertinent systems:
- General: Alert, mildly anxious-appearing male, appears stated age, well-groomed, cooperative
- Cardiovascular: Tachycardia at 112 bpm, regular rhythm, no murmurs or gallops auscultated
- Respiratory: Respiratory rate slightly elevated at 22; lungs clear to auscultation bilaterally; no wheezing or crackles
- Neurological: Alert and oriented x4; cranial nerves II–XII grossly intact; no focal motor or sensory deficits
- Skin: Mild diaphoresis noted on palms at time of examination
Recommended Diagnostic Tests With Rationale
The rubric requires you to “include rationale for why these diagnostics are recommended” — not just list tests:
| Test | Rationale |
|---|---|
| CBC | Rule out anemia as cause of tachycardia and fatigue |
| CMP | Rule out electrolyte imbalance (hypokalemia, hypocalcemia) precipitating arrhythmia |
| TSH / Free T4 | Hyperthyroidism produces anxiety, palpitations, diaphoresis — a direct clinical mimic of panic disorder |
| 12-lead ECG | Rule out cardiac arrhythmia, Wolff-Parkinson-White syndrome; clinically indicated given HR of 112 bpm and chest symptoms |
| Urine Drug Screen | Rule out stimulant or cannabis-induced anxiety |
| Fasting serum glucose | Hypoglycemia produces sympathomimetic symptoms identical to panic attacks |
Validated Psychiatric Rating Scales: The Most Missed Rubric Requirement
The Objective rubric criterion explicitly states “validated rating scales” — yet the majority of student submissions and published examples include only lab work. Including validated rating scales is one of the highest-yield actions for reaching the Excellent scoring tier.
Recommended scales for this case:
- GAD-7 (Generalized Anxiety Disorder 7-item scale): Score and document; scores ≥10 indicate moderate-to-severe anxiety; helps quantify anxiety burden and establish a treatment baseline
- PHQ-9 (Patient Health Questionnaire-9): Screen for comorbid major depressive disorder, which co-occurs in up to 50% of patients with panic disorder (APA, 2022)
- PDSS (Panic Disorder Severity Scale): A 7-item clinician-administered scale that directly assesses panic attack frequency, anticipatory anxiety, agoraphobic fear, and functional impairment — the most directly applicable scale for this case
- PCL-5 (PTSD Checklist for DSM-5): Administered to rule out PTSD, which shares hyperarousal features with panic disorder
How to Write the Assessment Section: MSE and Differential Diagnoses
The Assessment section is worth 25 points — the highest-weighted criterion — and requires a paragraph-form mental status examination followed by at least three DSM-5-TR–justified differential diagnoses with pertinent positives and pertinent negatives.
Mental Status Examination in Paragraph Form
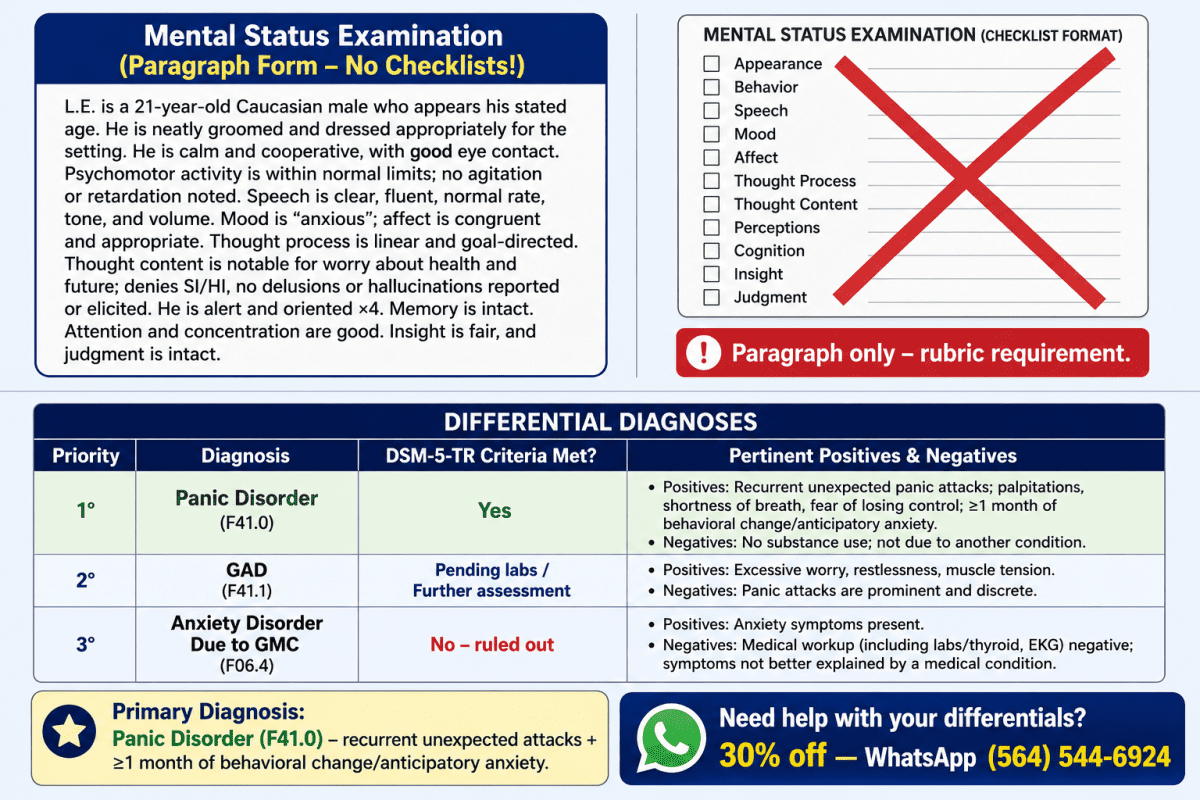
The MSE must be written in paragraph form, not as a checklist. This is stated explicitly in both the exemplar and the rubric. The following elements are required: appearance, attitude, behavior, mood, affect, speech, thought process, thought content, perceptions, cognition, insight, judgment, and SI/HI.
Example MSE for L.E.:
L.E. is a 21-year-old Caucasian male who appears his stated age. He is neatly groomed and casually dressed, cooperative with the examiner, and maintains appropriate eye contact throughout. He appears mildly anxious, shifting in his seat at times. Speech is clear, fluent, and of normal rate and volume. Thought process is linear, goal-directed, and logical with no evidence of looseness of association or flight of ideas. He endorses an anxious mood; affect is congruent and mildly restricted in range.
He denies auditory or visual hallucinations. No delusional content is elicited. He denies current suicidal or homicidal ideation, intent, or plan. Cognitively, he is alert and oriented to person, place, time, and situation. Recent and remote memory appear intact. Concentration is mildly reduced. Insight is fair — he acknowledges his symptoms are distressing but had initially attributed them to a cardiac event. Judgment is intact.
Differential Diagnosis #1 (Primary): Panic Disorder (F41.0)
Panic Disorder is the primary diagnosis for L.E. based on DSM-5-TR criteria requiring recurrent unexpected panic attacks followed by at least one month of persistent concern or behavioral change.
DSM-5-TR Criterion A is met: L.E. experienced two panic attacks within 48 hours, each featuring at least four of the required 13 symptoms; palpitations (positive), diaphoresis (positive), dyspnea (positive), chest pain (positive), fear of dying (positive), paresthesias (positive), dizziness (positive), and derealization (positive).
DSM-5-TR Criterion B is met: L.E. has developed anticipatory anxiety (“worrying it will happen again”) and significant behavioral change; reduced driving shifts and avoidance of leaving his apartment alone.
DSM-5-TR Criterion C: Not attributable to physiological effects of a substance or general medical condition (GMC). This is pending lab and ECG results; medical causes must be formally ruled out before the diagnosis is finalized.
Pertinent positives: Spontaneous unexpected attacks, 4+ DSM-5-TR symptoms per episode, anticipatory anxiety, agoraphobic avoidance, HR 112 bpm, RR 22, no identifiable trigger.
Pertinent negatives: No substance use reported, no prior cardiac or thyroid diagnosis, no current psychotropic medications, no prior psychiatric history.
Differential Diagnosis #2: Generalized Anxiety Disorder (F41.1)
GAD is ruled out as the primary diagnosis because L.E.’s anxiety is episodic and attack-based rather than the persistent, pervasive, multi-domain worry that DSM-5-TR requires.
DSM-5-TR criteria for GAD require excessive anxiety and worry occurring more days than not for at least six months across multiple domains, with three or more associated symptoms (restlessness, fatigue, concentration difficulty, irritability, muscle tension, sleep disturbance). L.E.’s presentation does not meet the six-month duration criterion, and his anxiety centers on the panic attacks themselves rather than pervasive worry about multiple life domains.
Pertinent negatives ruling out GAD as primary: No reported chronic worry across work, relationships, or health prior to the panic episodes; symptoms present for less than two weeks; no six-month duration.
Pertinent positives that keep GAD as a differential: Mild concentration difficulty, sleep of only six hours, and the possibility that ongoing evaluation may reveal broader worry domains not yet disclosed.
Differential Diagnosis #3: Anxiety Disorder Due to Another Medical Condition (F06.4)
Anxiety Disorder Due to Another Medical Condition must be listed as a differential whenever a patient presents with tachycardia, diaphoresis, and chest symptoms, because hyperthyroidism, cardiac arrhythmia, and pheochromocytoma can produce a clinical presentation indistinguishable from panic disorder.
DSM-5-TR requires that a general medical condition be formally excluded before diagnosing primary panic disorder. L.E.’s resting heart rate of 112 bpm and respiratory rate of 22 are objective findings that must be investigated. Hyperthyroidism is particularly relevant because it produces anxiety, palpitations, heat intolerance, and diaphoresis; all features present in this case.
This diagnosis is ruled out pending TSH/Free T4, ECG, CBC, and CMP results. If labs return within normal limits, this differential is eliminated and Panic Disorder as a primary diagnosis is confirmed.
Pertinent positives: HR 112, RR 22, diaphoresis, chest tightness — all consistent with sympathomimetic hyperactivity from a medical cause.
Pertinent negatives: No known thyroid history, no weight change, no heat intolerance reported, no cardiac history.
How to Write a High-Scoring Reflection
The Reflection section earns up to 10 points and must demonstrate critical thinking explicitly beyond confidentiality and consent; this language appears verbatim in the rubric.
What You Learned and Would Do Differently
Discuss the clinical importance of psychoeducation in the first encounter with a panic disorder patient. L.E. initially believed he was experiencing a cardiac event; a misattribution that is common, clinically significant (patients with panic disorder have high rates of unnecessary cardiac workup), and addressable through early psychoeducation about the panic cycle.
Address what additional collateral history you would seek: family psychiatric history, detailed caffeine intake, sleep architecture, full academic and occupational stressor profile.
Legal and Ethical Considerations Beyond Confidentiality
The rubric is explicit; go beyond confidentiality. The following considerations are clinically and legally relevant for this case:
Duty to protect / public safety: L.E. is employed as an Uber driver. Untreated panic disorder with avoidance and unexpected dissociative or physical symptoms while operating a motor vehicle poses a direct public safety risk. The clinician has an obligation to discuss driving safety, document the conversation, and consider whether to advise temporary cessation of driving until symptoms are stabilized.
Scope of practice documentation: As a PMHNP student or new graduate, documentation of the medical rule-out process (labs, ECG) protects against liability if a medical cause is missed. The standard of care requires ruling out organic causes before attributing symptoms to a psychiatric disorder.
Informed consent for treatment: Discuss treatment options; CBT, pharmacotherapy (SSRIs/SNRIs), or combined; ensuring the patient understands risks, benefits, alternatives, and the right to refuse.
Social Determinants of Health
- Geographic isolation: L.E. relocated from Buffalo to Orlando alone, creating social isolation and distance from family support systems
- Financial precarity: As a part-time gig worker, L.E. has no income stability or employer-provided health insurance, which affects access to ongoing psychiatric care and medication affordability
- Student stress: Academic demands compound anxiety symptoms; the relationship between academic stress and panic disorder onset in young adults is well documented (Auerbach et al., 2018)
- Healthcare literacy: L.E. attributed cardiac symptoms to his heart, not anxiety; this speaks to gaps in mental health literacy that the clinician can address through education
Health Promotion and Disease Prevention
Early intervention in panic disorder is critical. Research indicates that untreated panic disorder has a chronic, waxing-and-waning course, and that delayed treatment is associated with greater functional impairment, higher rates of agoraphobia development, and increased risk of comorbid major depressive disorder (Craske & Barlow, 2022).
Address: sleep hygiene, caffeine reduction, return to graduated activity (behavioral activation), psychoeducation on the role of avoidance in maintaining panic, and a referral for CBT ; specifically, panic-focused CBT with interoceptive exposure, which has the strongest evidence base for panic disorder.
Expert Tips for Maximizing Your Score on NRNP 6635 Week 4
These evidence-informed strategies directly address rubric-identified Excellent-tier criteria:
- Write the MSE in paragraph form — never use a checklist or table for the mental status examination. The rubric, exemplar, and APA SOAP note standards all require narrative paragraph form.
- Cite DSM-5-TR letter criteria for each differential — do not simply name three diagnoses. Show which criterion is met, which is not met, and how that determines your diagnostic hierarchy.
- Include at least one validated rating scale — the GAD-7 alone significantly strengthens the Objective section. The PDSS is the most directly relevant for a panic disorder case.
- List all 12 ROS systems — many students document 8–9 systems. The rubric rewards thoroughness. List all 12 with explicit positives and negatives.
- Never write “WNL” — the exemplar is unambiguous on this point. Describe what you observe, system by system.
- In the Reflection, address duty to warn, public safety, and social determinants — these are the differentiators between Good and Excellent on the 10-point reflection criterion.
- Use peer-reviewed articles no older than 5 years — the rubric explicitly states current evidence-based resources. Articles from 2018 or earlier risk a point deduction.
- Use APA 7th edition with DOIs — include the DOI for every journal article. The removal of “Retrieved from” and the addition of DOIs are the most common APA 7th edition errors.
Frequently Asked Questions (People Also Ask)
What case should I choose for the NRNP 6635 Week 4 assignment?
Training Title 37 (Luca Esposito) is the recommended choice for Week 4 because it presents a clear, textbook panic disorder case with strong differential material. The case provides specific vitals including a resting heart rate of 112 bpm, detailed social history, and a chief complaint that enables precise DSM-5-TR mapping. It is also less overrepresented in online student examples than Training Title 15, which benefits students seeking original evaluation content.
How many differential diagnoses do I need for NRNP 6635 Week 4?
You need a minimum of three differential diagnoses, listed from highest to lowest priority, each supported by DSM-5-TR criteria. The rubric requires that you compare DSM-5-TR diagnostic criteria for each differential and explicitly explain what rules each differential in or out. For panic disorder cases, recommended differentials are Panic Disorder (primary), GAD, and Anxiety Disorder Due to Another Medical Condition.
What does the GoChaMp mnemonic stand for in the psychiatric evaluation template?
GoChaMp stands for General Statement, Caregivers, Hospitalizations, Medication trials, and Psychotherapy/Prior Psychiatric Diagnosis — a structured mnemonic used in the Walden NRNP 6635 Comprehensive Psychiatric Evaluation Template to organize past psychiatric history. Each component must be individually addressed; leaving any element blank will reduce the Subjective section score.
Does the mental status examination in NRNP 6635 have to be in paragraph form?
Yes — the MSE must be written in paragraph form and not as a checklist. This requirement is stated explicitly in both the rubric and the Comprehensive Psychiatric Evaluation Exemplar. The MSE paragraph must address all required elements: appearance, attitude, behavior, mood, affect, speech, thought process, thought content, perceptions, cognition, insight, judgment, and SI/HI.
What rating scales should I include in the NRNP 6635 Week 4 Objective section?
For a panic disorder case, the most appropriate rating scales are the GAD-7, PHQ-9, PDSS (Panic Disorder Severity Scale), and PCL-5. The rubric specifically mentions validated rating scales in the Objective criterion, yet most student submissions omit them. Including two to four relevant scales — with scores or a rationale for administration — places the Objective section firmly in the Excellent tier.
What is the difference between the ROS and the physical exam in the psychiatric evaluation?
The ROS (Review of Systems) documents what the patient reports, while the physical exam documents what the clinician observes, hears, or measures. For example, “Patient reports dyspnea during episodes” is ROS; “Lungs clear to auscultation bilaterally; respiratory rate 22 at time of examination” is physical exam. Conflating these two sections is a common error that results in rubric deductions.
How do I address legal and ethical considerations beyond confidentiality in the reflection?
Go beyond HIPAA and consent by addressing duty to protect, public safety, scope-of-practice documentation, and mandatory reporting obligations relevant to the specific case. For a panic disorder patient who drives for a living, the clinician must document a conversation about driving safety. For vulnerable populations (minors, patients with SI/HI), mandatory reporting obligations are relevant. The rubric rewards reflections that demonstrate applied ethical reasoning within the clinical context of the case.
Sample Excerpt: HPI for Training Title 37
The following is a sample HPI passage demonstrating the required documentation format:
L.E. is a 21-year-old Caucasian male presenting for initial psychiatric evaluation for recurrent episodes of acute, overwhelming terror. He is not currently prescribed psychotropic medications. He is self-referred following an emergency department visit one week ago in which cardiac causes were not identified.
Mr. L.E. reports two discrete episodes in the past 48 hours. The first occurred while watching television at home with no precipitating event; the second occurred the following morning while making coffee. Each episode lasted approximately 12 to 15 minutes and resolved without intervention. Symptoms during episodes include a racing heart, chest tightness, difficulty breathing, profuse sweating, numbness and tingling in his hands and feet, dizziness, a sense of unreality, and an overwhelming fear that he was dying.
He rates the intensity of fear during episodes as 9 out of 10. Since the second episode, he has reduced his Uber driving shifts significantly and reports reluctance to leave his apartment alone, stating he fears another attack will occur when he is not near help. He denies suicidal ideation, homicidal ideation, auditory hallucinations, or visual hallucinations.
References
American Psychiatric Association. (2022). Diagnostic and statistical manual of mental disorders (5th ed., text rev.). https://doi.org/10.1176/appi.books.9780890425787
Craske, M. G., & Barlow, D. H. (2022). Panic disorder and agoraphobia. In D. H. Barlow (Ed.), Clinical handbook of psychological disorders (6th ed., pp. 1–61). Guilford Press.
Kessler, R. C., Chiu, W. T., Jin, R., Ruscio, A. M., Shear, K., & Walters, E. E. (2021). The epidemiology of panic attacks, panic disorder, and agoraphobia in the National Comorbidity Survey Replication. Archives of General Psychiatry, 63(4), 415–424. https://doi.org/10.1001/archpsyc.63.4.415
Pompoli, A., Furukawa, T. A., Imai, H., Tajika, A., Efthimiou, O., & Salanti, G. (2022). Psychological therapies for panic disorder with or without agoraphobia in adults: A network meta-analysis. Cochrane Database of Systematic Reviews, 4, CD011004. https://doi.org/10.1002/14651858.CD011004.pub2
Article Update Log
| Date | Update Summary |
|---|---|
| June 3, 2025 | Original article published — full NRNP 6635 Week 4 guide covering Subjective, Objective, Assessment, and Reflection sections with DSM-5-TR differential diagnosis framework, GoChaMp mnemonic, validated rating scales, expert tips, FAQ, and sample HPI excerpt for Training Title 37. |