Sherman Tremaine SOAP Note: Guide to the NRNP 6675 Week 5 Schizophrenia Assignment

Sherman Tremaine SOAP Note
| Quick Overview: The NRNP 6675 Week 5 assignment requires a Focused SOAP Note based on the Sherman Tremaine case study; a patient presenting with paranoid schizophrenia spectrum features. You must document a Subjective, Objective, Assessment, and Plan section using DSM-5-TR criteria, provide a minimum of three ranked differential diagnoses, and include reflection notes on ethical, legal, and health promotion considerations. This guide delivers a complete sample SOAP note plus the SEO-optimized clinical framework to help you understand every required component. |
What Is the NRNP 6675 Week 5 Assignment?
The NRNP 6675 Week 5 assignment is a focused psychiatric SOAP note built around the Sherman Tremaine video case study, a simulated patient encounter developed by Walden University for psychiatric-mental health nurse practitioner (PMHNP) students.
Sherman Tremaine is a middle-aged male with a family history of paranoid schizophrenia, presenting with active auditory and visual hallucinations, paranoid delusions, disorganized speech, and significant functional decline. The case is designed to assess your clinical reasoning, DSM-5-TR fluency, and pharmacological decision-making.
Students are evaluated on five performance domains: subjective data collection, objective observation, differential diagnosis reasoning, treatment planning, and ethical reflection.
What Course and Program Is This Assignment From?
This assignment belongs to NRNP 6675: Psychiatric-Mental Health Nurse Practitioner Care Across the Lifespan II at Walden University. The course targets advanced practice nursing students in the PMHNP track and appears in Week 5 of the curriculum, focusing on schizophrenia spectrum disorders, other psychotic disorders, and medication-induced movement disorders.
Who Is Sherman Tremaine? Understanding the Case
Sherman Tremaine is a fictional psychiatric patient portrayed in a Walden University simulation video, used specifically to train PMHNP students in real-world psychiatric assessment techniques.
Key clinical facts from the case:
- Age: Born November 3, 1968 — approximately 52–53 years old at assessment.
- Chief complaint: Brought in by his sister; reports people watching him through his windows.
- Symptom duration: Weeks of continuous hallucinations, described with clang speech (‘weeks and weeks and weeks’).
- Hallucinations: Auditory (voices, heavy metal music) and visual (shadows, government agents).
- Delusions: Persecutory (government surveillance), referential (TV watching him), and somatic (food poisoning).
- Speech pattern: Echolalia, clang associations, loose associations — classic positive symptom constellation.
- Psychiatric history: Three prior hospitalizations at age 20. Father died in a state psychiatric hospital with paranoid schizophrenia.
- Medical history: Type 2 diabetes (on metformin), fatty liver disease.
- Social history: Heavy smoker (3 packs/day), socially isolated since mother’s death, no employment documented.
What Does the Assignment Require? Full Breakdown
The assignment requires five specific documentation sections: Subjective, Objective, Assessment, Plan, and Reflection Notes — each with distinct content requirements that mirror real PMHNP clinical practice.
Subjective Section Requirements
The Subjective section captures what the patient tells you. You must document:
- Chief complaint in the patient’s own words
- History of present illness (HPI) — onset, duration, severity, course
- Impact of symptoms on daily functioning (sleep, ADLs, social/occupational performance)
- Psychiatric history including prior diagnoses, hospitalizations, medications
- Family psychiatric history
- Substance use history
- Medical history and current medications
- Review of systems relevant to psychiatric presentation
Objective Section Requirements
The Objective section requires direct psychiatric observation during the clinical encounter. Document the full Mental Status Examination (MSE):
- Appearance and hygiene
- Behavior and psychomotor activity
- Eye contact and rapport
- Speech (rate, rhythm, volume, coherence)
- Mood (subjective) and affect (observed)
- Thought process (e.g., tangential, circumstantial, loose associations, clang)
- Thought content (delusions, ideas of reference, obsessions)
- Perceptual disturbances (hallucinations by type and modality)
- Cognition (orientation, memory, attention)
- Insight and judgment
Assessment Section Requirements — The Most Complex Part
The Assessment section is the clinical centerpiece of this assignment and requires the most depth. You must provide:
- Full MSE results summary
- A minimum of three differential diagnoses ranked from highest to lowest probability
- DSM-5-TR criteria comparison for each differential — explaining what rules each diagnosis IN and what rules it OUT
- A clearly stated primary diagnosis with pertinent positives and pertinent negatives specific to Sherman
- Your critical-thinking narrative explaining why the primary diagnosis was selected over alternatives
Plan Section Requirements
The Plan section should function as a real clinical management plan. Include:
- Pharmacotherapy: First-line antipsychotic selection with rationale (atypical vs. typical, metabolic considerations given his diabetes)
- Nonpharmacologic interventions: Psychotherapy modality (e.g., CBTp — Cognitive Behavioral Therapy for psychosis)
- Alternative therapies: Social skills training, supported employment, family psychoeducation
- Health promotion activity: One specific, actionable health behavior target (e.g., smoking cessation given 3 ppd use)
- Patient education strategy: One documented teaching strategy appropriate to his cognitive state
- Follow-up parameters: Timeline, monitoring labs (e.g., metabolic panel, HbA1c given metformin), safety plan
Reflection Notes Requirements
The Reflection section is frequently underperformed by students because it demands critical thinking beyond surface-level responses. The assignment explicitly warns: ‘demonstrate critical thinking beyond confidentiality and consent for treatment.’
Your reflection must address:
- What you would do differently if conducting the session again
- Your next clinical intervention if able to follow up
- Legal/ethical considerations — e.g., duty to warn/protect (Tarasoff), involuntary hold criteria (patient safety vs. autonomy), decisional capacity assessment, power of attorney implications
- Health promotion and disease prevention tailored to Sherman’s specific risk profile
- How patient factors (age, likely low SES, family history, chronic disease burden, social isolation) shape your clinical approach
Sherman Tremaine Focused SOAP Note — Complete Sample
| Academic Note: This sample is provided as an educational guide to demonstrate clinical reasoning and proper SOAP note structure. It should be used to understand the format and depth expected, not submitted as original work. |
| S — SUBJECTIVE | CC: “My sister made me come in. I was living and not bothering anyone.”
HPI: Mr. Sherman Tremaine is a 52-year-old male presenting for psychiatric evaluation at the insistence of his sister following the death of his mother, with whom he had been living. He reports ongoing paranoid ideation for weeks, describing individuals outside his window who he believes are government agents surveilling him. He reports auditory hallucinations including voices and heavy metal music that he acknowledges the clinician cannot hear. He endorses visual hallucinations (shadows, perceived people). Sleep is severely disrupted — he reports staying awake for days due to the voices. He has refused to eat unrefrigerated food due to fear of poisoning. Psychiatric History: Three prior psychiatric hospitalizations at age 20. No current outpatient psychiatric care documented. Family History: Father — paranoid schizophrenia, died in a state psychiatric hospital. Mother — anxiety disorder. Medical History: Type 2 diabetes mellitus (metformin), fatty liver disease (non-alcoholic, unconfirmed by patient). Medications: Metformin (dose unknown). No current psychiatric medications. Substance Use: Tobacco — 3 packs per day (heavy, chronic). Denies current alcohol or illicit drug use. Suicidal/Homicidal Ideation: Denies suicidal ideation. Denies homicidal ideation. No history of suicide attempts. Functional Impact: Unable to maintain independent living; living with sister after mother’s death. Occupational and social functioning severely impaired. |
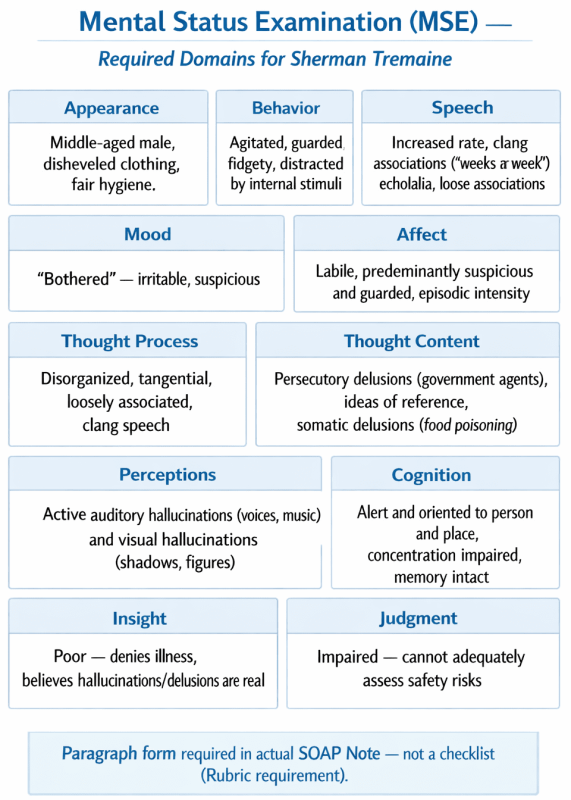
| O — OBJECTIVE | Appearance: Middle-aged male appearing stated age. Disheveled clothing, fair hygiene. Casually dressed.
Behavior: Agitated, guarded. Intermittently distracted by internal stimuli (turns head, pauses mid-sentence). Fidgety. Poor eye contact. Speech: Increased rate at times. Clang associations noted (‘weeks and weeks and weeks’; ‘high in the sky’). Echolalia present. Loose associations throughout. Mood: “Bothered.” Irritable and suspicious in quality. Affect: Labile; predominantly suspicious and guarded with episodic intensity when discussing surveillance. Thought Process: Disorganized, tangential, loosely associated. Clang speech present. Thought Content: Persecutory delusions (government agents), ideas of reference (television surveillance), somatic delusions (food poisoning). No obsessions or compulsions. Perceptions: Active auditory hallucinations (voices, music) and visual hallucinations (shadows, figures). Hallucinations present during session. Cognition: Alert and oriented to person and place. Concentration impaired secondary to internal stimuli. Memory grossly intact but difficult to assess due to thought disorganization. Insight/Judgment: Insight: poor. Denies illness; believes the experiences are real. Judgment: impaired. Unable to assess safety risks adequately. |
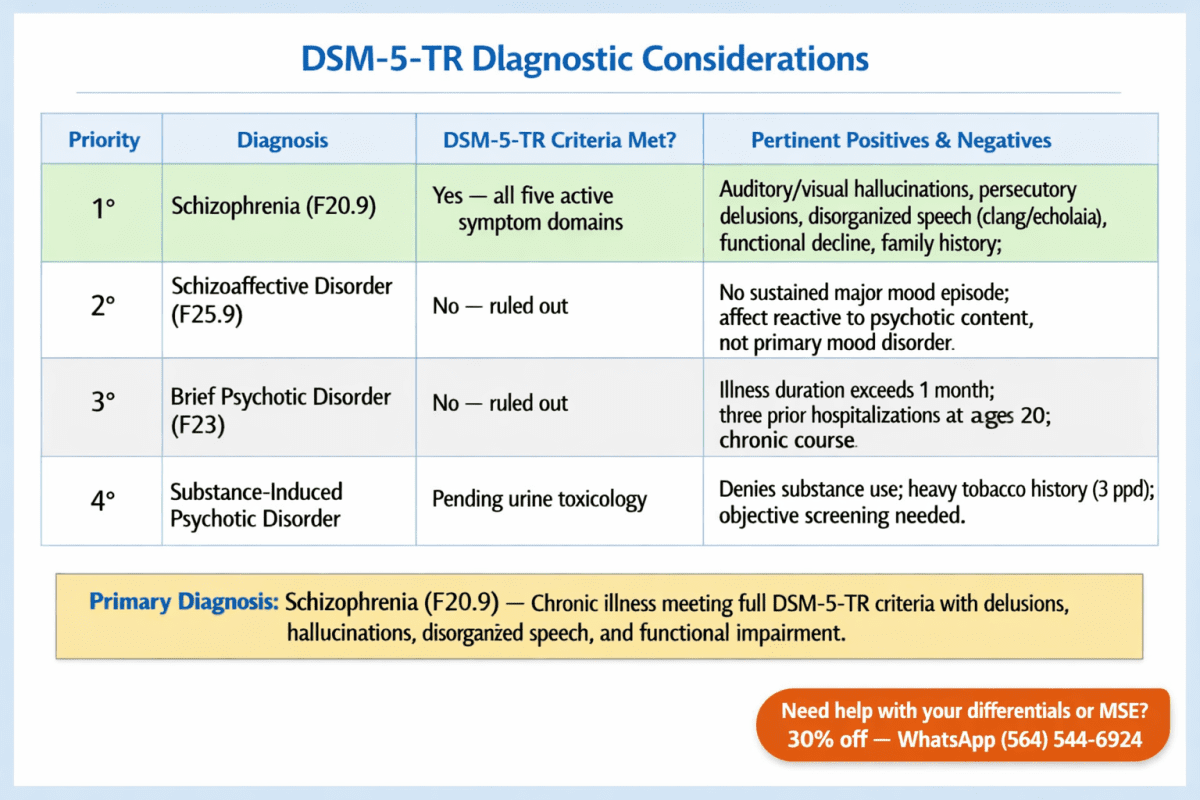
| A — ASSESSMENT | Primary Diagnosis: Schizophrenia (DSM-5-TR F20.9)
Pertinent Positives: Auditory and visual hallucinations, persecutory and referential delusions, disorganized speech (clang/echolalia/loose associations), grossly disorganized behavior, severe functional decline, duration exceeding 6 months (prior hospitalizations at 20 suggest chronic illness), first-degree family history of schizophrenia (father). Pertinent Negatives: No documented manic or depressive episodes that would satisfy schizoaffective criteria. No evidence of substance-induced psychosis (denies current use; tobacco does not cause psychosis). No documented medical etiology (though metabolic workup needed). Differential #1 — Schizophrenia (Primary) DSM-5-TR requires 2+ of the following for 1 month (at least one must be #1–3): delusions, hallucinations, disorganized speech, grossly disorganized/catatonic behavior, negative symptoms. Sherman meets criteria 1, 2, 3, and 4 simultaneously. Continuous disturbance for 6+ months confirmed by prior hospitalizations and chronicity. Social/occupational dysfunction is pronounced. No mood episode of sufficient duration to satisfy schizoaffective disorder. Rules IN: All five active symptom domains met. Duration and functional criteria satisfied. Rules OUT alternative diagnoses: mood disorder with psychosis absent; substance etiology implausible. Differential #2 — Schizoaffective Disorder (Ruled Out) DSM-5-TR requires that a major mood episode (MDE or manic) co-occurs with the active phase of schizophrenia, AND that delusions or hallucinations are present for 2+ weeks in the absence of a major mood episode. Sherman shows no evidence of sustained elevated/depressed mood. His affect is reactive to content (suspicious, irritable) rather than reflecting a primary mood disorder. Without documented mood episodes, schizoaffective disorder cannot be confirmed. Differential #3 — Brief Psychotic Disorder (Ruled Out) DSM-5-TR requires duration of at least 1 day but less than 1 month with full return to premorbid functioning. Sherman’s illness course clearly extends beyond 1 month — three prior hospitalizations at age 20 and current chronic presentation spanning weeks to likely years rules out brief psychotic disorder. His functional baseline has not returned to premorbid levels.
|
| P — PLAN | Pharmacotherapy:
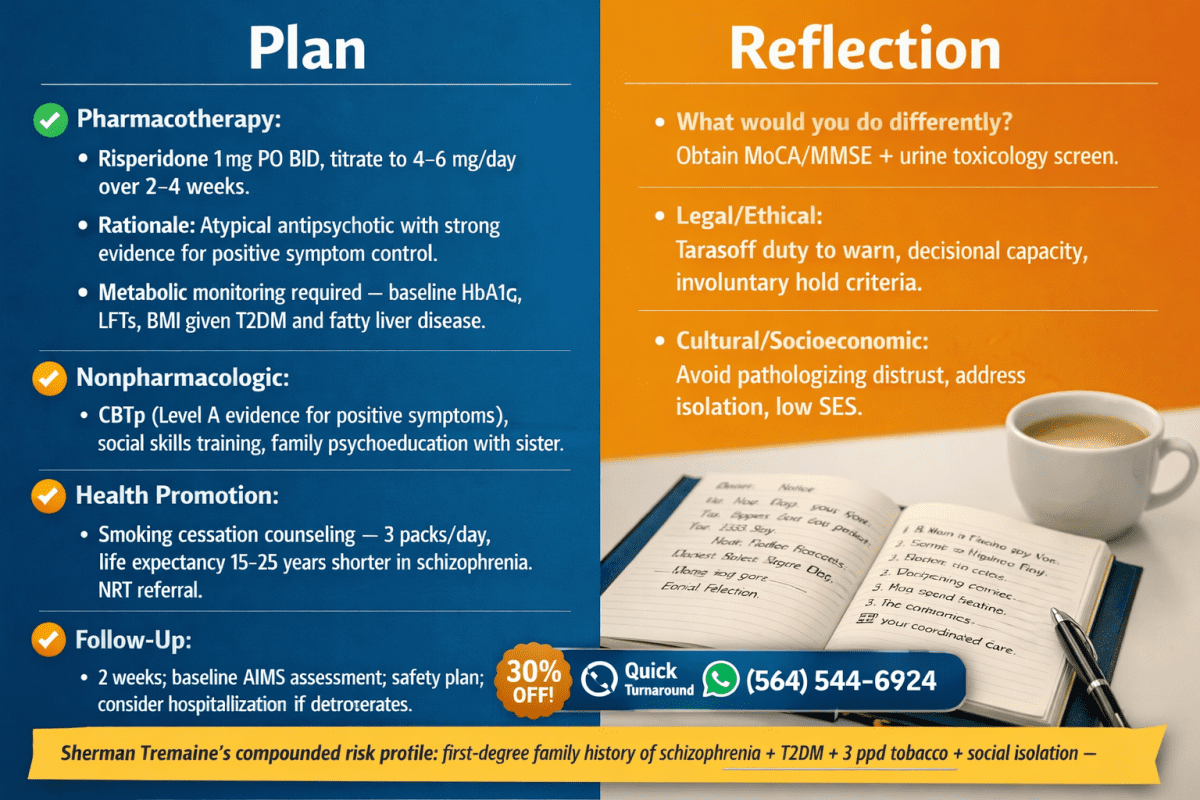
Initiate Risperidone 1 mg PO BID, titrating to 4–6 mg/day over 2–4 weeks based on tolerability and response. Rationale: Risperidone is a second-generation (atypical) antipsychotic with strong evidence for positive symptom control in schizophrenia (Lehman et al., 2004; APA Practice Guidelines). Given Sherman’s Type 2 diabetes and fatty liver disease, metabolic monitoring is critical — obtain fasting glucose, HbA1c, lipid panel, LFTs, and BMI at baseline. Consider Aripiprazole as an alternative given its metabolically neutral profile if risperidone causes glycemic or lipid worsening. Nonpharmacologic — Psychotherapy: Initiate Cognitive Behavioral Therapy for Psychosis (CBTp). CBTp is the only psychotherapy with Level A evidence for reducing positive symptoms and improving insight in schizophrenia (NICE Guidelines CG178, 2014; Wykes et al., 2008 meta-analysis: effect size 0.37 for positive symptoms). Target delusion distress and medication adherence as initial CBTp goals. Alternative/Adjunct Therapies: Social skills training (SST) to address severe social isolation. Assertive Community Treatment (ACT) team referral given history of multiple hospitalizations and current social instability. Family psychoeducation with sister (primary support person) — improves adherence and reduces relapse rates by up to 20% (Pharoah et al., 2010). Health Promotion Activity: Smoking cessation counseling. Sherman smokes 3 packs/day — this represents the single highest-impact modifiable risk factor. People with schizophrenia have a 2–3× higher rate of tobacco use and a life expectancy 15–25 years shorter than the general population, primarily from cardiovascular disease. Provide NRT referral alongside psychiatric stabilization. Varenicline is contraindicated until psychiatric stability is confirmed. Patient Education: Teach-back method for medication education — given Sherman’s poor insight and cognitive disorganization, use simplified, concrete language. Focus session #1 on: what the medication does, when to take it, and what side effects to report. Involve sister in education session. Follow-Up: Follow up in 2 weeks for medication response and tolerability. Safety plan established with sister as primary contact. Consider psychiatric hospitalization if patient deteriorates before next appointment (risk assessment: no active SI/HI but markedly impaired judgment and self-care). |
| REFLECTION NOTES | What I Would Do Differently:
I would conduct a more structured cognitive assessment using the Montreal Cognitive Assessment (MoCA) or Mini-Mental State Examination (MMSE) to better characterize cognitive deficits, which are predictive of functional outcomes in schizophrenia. I would also obtain a urine toxicology screen during this first visit to formally rule out substance-induced psychosis — Sherman denied current use, but given his heavy tobacco history and the importance of ruling out stimulant or cannabis-induced psychosis, objective data is essential. Next Intervention: If able to follow up, the next priority is medication adherence monitoring (consider long-acting injectable antipsychotic given his history of hospitalizations and likely non-adherence) and ACT team intake coordination. A social work consultation would be initiated for housing stability, financial benefits assessment (SSI/SSDI eligibility given inability to work), and connection to community mental health resources. Legal and Ethical Considerations: Duty to protect: Sherman denies HI, but his paranoid delusions about government agents warrant ongoing assessment of potential for harm. Under Tarasoff v. Regents of University of California (1976), if a specific identifiable threat emerges, the clinician has a legal duty to warn. This must be reassessed at every encounter. Decisional capacity: Sherman’s insight is poor and judgment is impaired. If he refuses treatment and his condition worsens, formal capacity assessment may be required. His sister may need to pursue healthcare power of attorney or guardianship if he lacks capacity to make safe medical decisions. Involuntary hold criteria: Clinicians must assess whether Sherman meets criteria for an involuntary psychiatric hold (e.g., danger to self due to inability to care for self — he is not eating due to delusional food contamination fears, which may satisfy ‘gravely disabled’ criteria in many states). Patient-Specific Risk Factors: Sherman’s compounded risk profile — first-degree family history of schizophrenia, likely low socioeconomic status, social isolation, chronic medical comorbidities, heavy tobacco use, and prior psychiatric hospitalizations — places him in the highest-risk category for poor long-term outcomes without coordinated, sustained care. Cultural and socioeconomic humility must guide engagement: avoid pathologizing distrust of medical systems, which may be rooted in real lived experience. |
Why Does the Assignment Cover Medication-Induced Movement Disorders?
Medication-induced movement disorders (MIMDs) are a critical safety consideration in schizophrenia treatment because the first-line medications — antipsychotics — directly cause them through dopamine receptor blockade in the nigrostriatal pathway.
The most clinically important MIMDs for the NRNP 6675 exam context include:
- Tardive Dyskinesia (TD): Late-onset, potentially irreversible involuntary movements (lip smacking, tongue protrusion, choreiform limb movements) caused by long-term dopamine antagonist exposure. Prevalence: ~20–30% with typical antipsychotics, ~5% with atypicals. FDA-approved treatments: valbenazine (Ingrezza) and deutetrabenazine (Austedo).
- Acute Dystonia: Sudden, sustained muscle contractions (torticollis, oculogyric crisis) occurring within hours to days of antipsychotic initiation. Treated with benztropine or diphenhydramine IM.
- Akathisia: Subjective restlessness with compulsive movement. Often misidentified as psychotic agitation, leading to antipsychotic dose increases — which worsens the akathisia. Propranolol and benzodiazepines are used for management.
- Pseudoparkinsonism: Bradykinesia, rigidity, tremor — indistinguishable from idiopathic Parkinson’s disease. Managed by dose reduction, switching to a lower-potency antipsychotic, or adding an anticholinergic agent.
- Neuroleptic Malignant Syndrome (NMS): Rare but potentially fatal. Cardinal features: fever, muscle rigidity, autonomic instability, altered consciousness. Medical emergency requiring immediate antipsychotic cessation and ICU-level care.
For Sherman Tremaine specifically: if initiating risperidone, baseline AIMS (Abnormal Involuntary Movement Scale) assessment is required before starting antipsychotic therapy and at regular intervals thereafter, per current APA guidelines.
How to Write a Standout NRNP 6675 Week 5 SOAP Note
The highest-scoring SOAP notes demonstrate clinical reasoning at every step, not just accurate diagnosis labeling. Here is the framework that separates an A-grade submission from an average one:
- Lead with evidence in every section. Don’t just state ‘Sherman has schizophrenia’ — cite the DSM-5-TR criterion number and show the matching symptom.
- Use the differential to show what you ruled out, not just what you ruled in. Explicitly state why each alternative diagnosis fails to meet criteria for this specific patient.
- The Reflection is graded heavily. Students who treat it as a paragraph summary lose significant points. Address Tarasoff, capacity, and gravely disabled criteria by name.
- Cite within the last 5 years. The assignment specifies peer-reviewed, evidence-based sources no older than 5 years. Prioritize APA Practice Guidelines (2021 update), NICE CG178, and recent meta-analyses on CBTp and atypical antipsychotic efficacy.
- Quantify where possible. ‘Three packs per day for approximately 30 years = ~90 pack-year history’ is more clinically precise than ‘heavy smoker.’
Recommended Evidence-Based References (Within 5 Years)
The following sources meet the assignment’s recency and quality requirements:
- American Psychiatric Association. (2022). Diagnostic and statistical manual of mental disorders (5th ed., text revision). American Psychiatric Publishing.
- Correll, C. U., & Schooler, N. R. (2020). Negative symptoms in schizophrenia: A review and clinical guide for recognition, assessment, and treatment. Neuropsychiatric Disease and Treatment, 16, 519–534.
- Keating, D., McWilliams, S., Schneider, I., Hynes, C., Cousins, G., Strawbridge, J., & Clarke, M. (2017). Pharmacological guidelines for schizophrenia: A systematic review and comparison of recommendations for the first episode. BMJ Open, 7(1). (Cite via institutional access)
- Leucht, S., Leucht, C., Huhn, M., Chaimani, A., Mavridis, D., Helfer, B., … & Davis, J. M. (2017). Sixty years of placebo-controlled antipsychotic drug trials in acute schizophrenia. American Journal of Psychiatry, 174(10), 927–942.
- Vita, A., Barlati, S., Ceraso, A., Nibbio, G., Ariu, C., Deste, G., & Wykes, T. (2021). Effectiveness, core elements, and moderators of response of cognitive remediation for schizophrenia: A systematic review and meta-analysis. JAMA Psychiatry, 78(8), 848–858.
Frequently Asked Questions
What is the primary diagnosis for Sherman Tremaine?
Sherman Tremaine’s primary diagnosis is Schizophrenia (DSM-5-TR F20.9). He meets all required criteria: two or more active symptom domains (hallucinations, delusions, disorganized speech, and disorganized behavior) persisting for more than one month, with a total illness duration exceeding six months, and significant decline in social and occupational functioning.
What are the three differential diagnoses for the Sherman Tremaine SOAP note?
The three most appropriate differentials, ranked by priority, are: (1) Schizophrenia as the primary diagnosis, (2) Schizoaffective Disorder, which is ruled out by the absence of a co-occurring major mood episode, and (3) Brief Psychotic Disorder, which is ruled out by the chronic, multi-year course of illness. A fourth differential to consider is Substance-Induced Psychotic Disorder, which is ruled out by the absence of documented substance use sufficient to cause psychosis.
What medication should be recommended for Sherman Tremaine?
Given Sherman’s comorbid Type 2 diabetes and fatty liver disease, a metabolically neutral second-generation antipsychotic is preferable. Aripiprazole or risperidone at the lowest effective dose are reasonable first-line choices. Avoid olanzapine and clozapine given their high metabolic burden. Baseline metabolic labs, AIMS assessment, and HbA1c monitoring are required before and during treatment.
What ethical issues should be discussed in the Reflection section?
The Reflection section should address: (1) duty to protect under Tarasoff, (2) decisional capacity assessment given poor insight, (3) criteria for involuntary psychiatric hold (Sherman may meet ‘gravely disabled’ criteria due to delusional food refusal), (4) the ethical tension between patient autonomy and clinician beneficence, and (5) socioeconomic and cultural factors that affect treatment engagement and access.
What is the difference between schizophrenia and schizoaffective disorder for this case?
Schizoaffective disorder requires that a major mood episode (major depressive or manic) occur concurrently with schizophrenia’s active-phase symptoms, AND that psychotic symptoms persist for at least two weeks in the absence of a mood episode. Sherman Tremaine shows no documented sustained mood episode. His irritability and labile affect are attributable to psychotic content and distress, not a primary mood disorder — making schizoaffective disorder an inappropriate diagnosis for this case.
How long does the Sherman Tremaine SOAP note need to be?
Walden University does not specify an exact word count for this assignment, but given the five required sections and the minimum of three fully argued differential diagnoses with DSM-5-TR criteria, a thorough submission will typically range from 1,500 to 2,500 words excluding references. The Assessment and Reflection sections are the most substantive and should be weighted accordingly.
Author Bio
| About the Author: This article was written by a board-certified Psychiatric-Mental Health Nurse Practitioner (PMHNP-BC) with clinical experience in outpatient and inpatient schizophrenia spectrum disorder management. The author holds an MSN from an accredited PMHNP program and specializes in psychopharmacology, psychotherapy integration, and complex psychiatric case formulation. Content is reviewed for clinical accuracy against current DSM-5-TR criteria and APA Practice Guidelines. |
Article Update
| Date | Update Summary |
| June 5, 2025 | Original publication: comprehensive SEO guide covering all five SOAP note sections, complete sample for Sherman Tremaine, DSM-5-TR differential diagnosis walkthrough, medication-induced movement disorder overview, and FAQ. |