NRNP/PRAC 6665 & 6675 Focused SOAP Note for PMHNP Students: Expert Guide, Worked Example & Video Case Presentation Tips

NRNP/PRAC 6665 & 6675 Focused SOAP Note for PMHNP Students
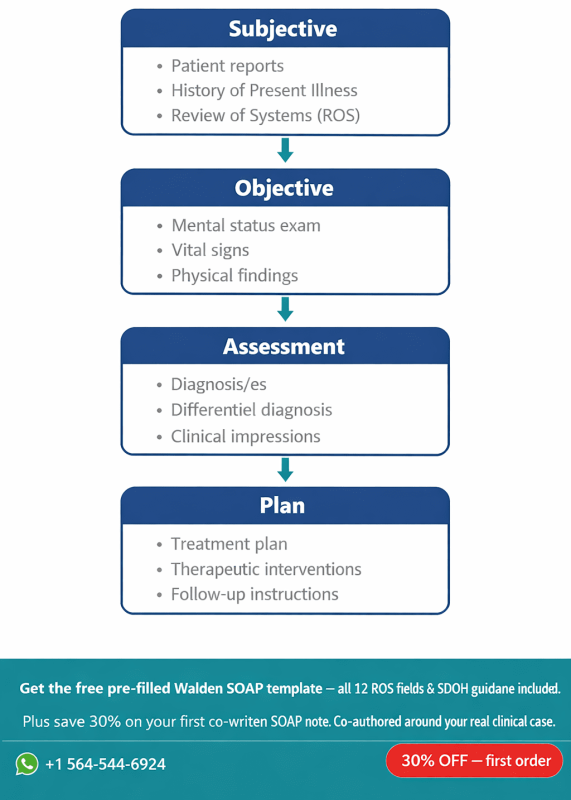
Quick Overview: The NRNP/PRAC 6665 & 6675 Focused SOAP Note assignment requires you to document a real psychiatric patient using Walden’s four-section template (Subjective, Objective, Assessment, Plan), obtain a wet preceptor signature, and record an 8-minute video case consultation. This guide walks you through every section, provides a complete worked fictional example, and explains exactly what earns full marks.
If you are a working nurse juggling back-to-back clinical shifts while completing your Psychiatric Mental Health Nurse Practitioner (PMHNP) practicum at Walden University, this assignment is one of the highest-stakes weekly deliverables you will face. Faculty evaluate your ability to think like an advanced psychiatric provider, not just document like a floor nurse.
Two files must reach the submission portal on time: your SOAP note (Word document plus a preceptor-signed PDF) and your Kaltura video. Missing either one triggers automatic point deductions under Walden’s grading policy. Read this guide before you open the template.
To Prepare
- Review the Kaltura buttonfrom the Classroom Support Center (accessed via the Help button) for help creating your self-recorded Kaltura video.
- Select a child or adolescent patient that you examined during the last 3 weeks who presented with a disorder for which you have not already created a Focused SOAP Note in Weeks 3 or 7. (For instance, if you selected a patient with anorexia nervosa in Week 7, you must choose a patient with another type of disorder for this week.)
- Create a Focused SOAP Note on this patient using the template provided in the Learning Resources. There is also a completed Focused SOAP Note Exemplar provided to serve as a guide to assignment expectations.
Please Note:- All SOAP notes must be signed by your Preceptor. Note: Electronic signatures are not accepted.
- When you submit your note, you should include the complete focused SOAP note as a Word document and PDF/images of the completed assignment signed by your Preceptor.
- You must submit your SOAP note using Turnitin. Note: If both files are not received by the due date, faculty will deduct points per the Walden Grading Policy.
- Then, based on your SOAP note of this patient, develop a video case study presentation. Take time to practice your presentation before you record.
- Include at least five scholarly resources to support your assessment, diagnosis, and treatment planning.
- Ensure that you have the appropriate lighting and equipment to record the presentation.
The Assignment
Record yourself presenting the complex case for your clinical patient.
Do not sit and read your written evaluation! The video portion of the assignment is a simulation to demonstrate your ability to succinctly and effectively present a complex case to a colleague for a case consultation. The written portion of this assignment is a simulation for you to demonstrate to the faculty your ability to document the complex case as you would in an electronic medical record. The written portion of the assignment will be used as a guide for faculty to review your video to determine if you are omitting pertinent information or including non-essential information during your case staffing consultation video.
In your presentation:
- Dress professionally and present yourself in a professional manner.
- Display your photo ID at the start of the video when you introduce yourself.
- Ensure that you do not include any information that violates the principles of HIPAA (i.e., don’t use the patient’s name or any other identifying information).
- Present the full complex case study. Include chief complaint; history of present illness; any pertinent past psychiatric, substance use, medical, social, family history; most recent mental status exam; current psychiatric diagnosis including differentials that were ruled out; and plan for treatment and management.
- Report normal diagnostic results as the name of the test and “normal” (rather than specific value). Abnormal results should be reported as a specific value.
- Be succinct in your presentation, and do not exceed 8 minutes. Specifically address the following for the patient, using your SOAP note as a guide:
- Subjective: What details did the patient provide regarding their chief complaint and symptomology to derive your differential diagnosis? What is the duration and severity of their symptoms? How are their symptoms impacting their functioning in life?
- Objective: What observations did you make during the psychiatric assessment?
- Assessment:Discuss their mental status examination results. What were your differential diagnoses? Provide a minimum of three possible diagnoses and why you chose them. List them from highest priority to lowest priority. What was your primary diagnosis, and why? Describe how your primary diagnosis aligns with DSM-5diagnostic criteria and supported by the patient’s symptoms.
- Plan:In your video, describe your treatment plan using clinical practice guidelines supported by evidence-based practice. Include a discussion on your chosen FDA-approved psychopharmacologic agents and include alternative treatments available and supported by valid research. All treatment choices must have a discussion of your rationale for the choice supported by valid research. What were your follow-up plan and parameters? What referrals would you make or recommend as a result of this treatment session?
- In your written plan include all the above as well as include one social determinant of health according to the HealthyPeople 2030 (you will need to research) as applied to this case in the realm of psychiatry and mental health. As a future advanced provider, what are one health promotion activity and one patient education consideration for this patient for improving health disparities and inequities in the realm of psychiatry and mental health? Demonstrate your critical thinking.
- Reflection notes:What would you do differently with this patient if you could conduct the session over? If you are able to follow up with your patient, explain whether these interventions were successful and why or why not. If you were not able to conduct a follow up, discuss what your next intervention would be.
What Is the NRNP/PRAC 6665 & 6675 Focused SOAP Note Assignment?
The Focused SOAP Note is a practicum documentation assignment designed to replicate real-world psychiatric clinical charting while simultaneously demonstrating academic competency in DSM-5-TR diagnosis, evidence-based pharmacology, and patient-centered care planning.
Walden’s PRAC 6665 (PMHNP Care Across the Lifespan I) and PRAC 6675 (Lifespan II) share the same Comprehensive Focused SOAP Psychiatric Evaluation Template, revised December 2022. Both courses require you to select a patient you personally examined within the previous three weeks at your Meditrek-approved clinical site.
The assignment has two inseparable components:
- The written SOAP note submitted as a Word document and a PDF, both bearing your preceptor’s physical (wet) signature on every page. Electronic signatures are not accepted.
- The video case presentation recorded through Kaltura, capped at eight minutes, in which you present the case as if consulting with a clinical colleague.
Faculty expectation: The video is not a recitation of your written note. It simulates real case-staffing consultation. Faculty use your written note to check whether you omit clinically significant information or include irrelevant detail during the oral presentation.
Who Selects the Patient?
You select the patient. The only restrictions are that the patient must be someone you examined personally in the last three weeks, and you cannot reuse a disorder category you already documented in Weeks 3 or 7 of the same course. For PRAC 6665 and 6675, any age is eligible; NRNP 6660 (Child and Adolescent) restricts selection to pediatric patients.
How to Complete Each Section of the Walden SOAP Template
Each of the four SOAP sections carries distinct faculty expectations that go beyond basic clinical charting. Knowing what evaluators are actually looking for inside each field is how you convert a competent note into a high-scoring one.
Subjective: Capturing the Patient’s Story with Clinical Precision
The Subjective section opens with the chief complaint (CC) in the patient’s own words, placed inside quotation marks. Follow this immediately with a structured History of Present Illness (HPI) that addresses onset, duration, severity, quality, modifying factors, and functional impact. Aschenbrenner and Venable (2021) note that psychiatric HPI documentation must establish a temporal narrative rather than a symptom checklist.
Required Subjective fields in the Walden template:
- CC — verbatim patient statement in quotation marks
- HPI — structured narrative including duration, severity, and functional impairment across settings
- Substance Current Use — quantity, frequency, and date of last use for each substance
- Medical History — current medications with dosages, allergies, and reproductive history
- Review of Systems (ROS) — 12-system review with each system individually addressed
The ROS is where many students lose points by writing ‘denies all’ as a blanket statement. Faculty expect you to address each system individually, even if findings are negative. The template lists: General, HEENT, Skin, Cardiovascular, Respiratory, Gastrointestinal, Genitourinary, Neurological, Musculoskeletal, Hematologic, Lymphatics, and Endocrinologic.
Objective: Documenting What You Observed
The Objective section in psychiatric SOAP notes centers on the Mental Status Examination (MSE), not physical vital signs alone. Carlat (2024) describes the MSE as the psychiatric equivalent of a physical exam, covering appearance, behavior, speech, mood (patient’s words), affect (your observation), thought process, thought content, perceptual disturbances, cognition, insight, and judgment.
For Diagnostic results, Walden’s instructions are specific: report normal results as the test name followed by ‘normal.’ Report abnormal results with the actual value. For example: ‘TSH normal; fasting glucose 142 mg/dL (elevated).’
Assessment: Building a Defensible Diagnostic Impression
The Assessment section is the intellectual centerpiece of the note and the section most scrutinized during faculty review. You are required to provide a minimum of three differential diagnoses, ranked from highest to lowest priority, with a written rationale for each.
Your primary diagnosis must be justified against DSM-5-TR criteria (American Psychiatric Association, 2022). This means you cite specific criterion sets, not general descriptions. For example, stating that a patient meets Criteria A through E for Major Depressive Disorder, Single Episode, Moderate (F32.1) is far stronger than stating ‘the patient appears depressed.’
Required Assessment components:
- MSE summary — brief interpretive synthesis of your objective findings
- Differential #1 (primary) — diagnosis with DSM-5-TR code, criteria mapping, and rationale for selection
- Differential #2 — second-most likely diagnosis and why it ranks below the primary
- Differential #3 — ruled-out diagnosis with explicit reasoning for exclusion
- Reflections — initial clinical impressions and self-assessment of diagnostic reasoning process
Pro tip: Students who rank diagnoses without explaining why they ruled out competing options consistently score lower. Write ‘Differential #2 was deprioritized because X criterion was not met’ rather than simply listing three diagnoses.
Plan: Where Evidence-Based Practice Meets Patient-Centered Care
The Case Formulation and Treatment Plan must satisfy multiple faculty evaluation criteria simultaneously. Stahl (2021) emphasizes that psychopharmacologic treatment decisions should always be justified against the mechanism of action, the patient’s comorbidity profile, and existing clinical practice guidelines.
Your Plan must address the following in writing:
- FDA-approved pharmacologic agent(s) — drug name, dose, frequency, rationale, and mechanism of action
- Alternative treatments — at least one non-pharmacologic option supported by peer-reviewed evidence
- Follow-up parameters — specific timeframes, monitoring targets, and clear criteria for medication adjustment
- Referrals — any specialist, therapy modality, or community resource recommended
- Social Determinant of Health (SDOH) — one SDOH from Healthy People 2030 applied to this patient’s case
- Health promotion activity — one evidence-based recommendation addressing health disparities for this population
- Patient education — specific psychoeducation content delivered or planned during this visit
- Reflection notes — what you would do differently, or follow-up outcome if a return visit occurred
The SDOH requirement distinguishes this assignment from standard clinical SOAP formats. Healthy People 2030 identifies five SDOH domains: Economic Stability, Education Access, Health Care Access, Neighborhood Environment, and Social and Community Context (U.S. DHHS, 2022). Choose the domain most relevant to your patient’s presentation and describe how it affects their psychiatric prognosis.
Complete Worked Example: Focused SOAP Note for Adolescent ADHD with Comorbid Anxiety
The following is a fictional, HIPAA-compliant worked example written to Walden’s PRAC 6665/6675 template standard. All patient details are fabricated for educational purposes. This example targets a common child/adolescent psychiatric presentation to illustrate the depth of documentation expected.
Subjective
CC: “I can’t sit still in class and my mom says I’m always worried about everything.”
HPI: J.M. is a 12-year-old Hispanic male referred by his pediatrician following a school-based behavioral evaluation. He presents to the outpatient psychiatric clinic accompanied by his mother. Symptoms of inattention, hyperactivity, and excessive worry have been present for approximately three years according to parent and teacher report. The patient states he “can never finish his homework without getting distracted” and describes difficulty falling asleep due to racing thoughts about upcoming tests. Symptoms are present in at least two settings (home and school), consistent with the DSM-5-TR cross-situational criterion for ADHD. Functioning is impaired in academic performance (current GPA 2.1, down from 3.4 two years ago) and peer relationships. No history of mood episodes, psychosis, or suicidal ideation.
Substance Current Use: Denied by patient. Mother denies any known substance exposure.
- Current Medications: None.
- Allergies: Penicillin (rash).
- Reproductive History: Not applicable (pre-pubertal).
ROS:
- General: Positive for fatigue and sleep-onset difficulty. No fever or weight changes.
- HEENT: Negative.
- Skin: Negative.
- Cardiovascular: Negative.
- Respiratory: Negative.
- Gastrointestinal: Positive for occasional stomachaches described as “butterflies” before school.
- Genitourinary: Negative.
- Neurological: Positive for tension-type headaches (1 to 2 per week).
- Musculoskeletal: Negative.
- Hematologic: Negative.
- Lymphatics: Negative.
- Endocrinologic: Negative.
Objective
Diagnostic Results: CBC normal; lead level normal; TSH normal. Vanderbilt Assessment Scale (parent and teacher forms) positive for combined-type ADHD symptom profile scoring above clinical threshold on both inattention and hyperactivity/impulsivity subscales. Generalized Anxiety Disorder-7 (GAD-7) score: 12 (moderate anxiety).
Mental Status Examination:
- Appearance: Well-groomed, age-appropriate dress, appears stated age.
- Behavior: Restless, frequently shifts in chair, intermittent eye contact.
- Speech: Rapid rate, normal volume, slightly tangential at times.
- Mood: “Pretty stressed, I guess.”
- Affect: Mildly anxious, mood-congruent.
- Thought process: Linear but easily derailed by minor environmental stimuli.
- Thought content: No suicidal ideation, no homicidal ideation, no delusions.
- Perceptual disturbances: Denied hallucinations in all modalities.
- Cognition: Oriented x4. Attention impaired on serial 7s task.
- Insight: Fair; patient acknowledges difficulty concentrating but minimizes functional impact.
- Judgment: Good for developmental age.
Assessment
Diagnostic Impression:
- Differential #1 — Attention-Deficit/Hyperactivity Disorder, Combined Presentation, F90.2 (Primary). J.M. meets DSM-5-TR Criteria A through E for ADHD Combined Type: six or more inattention symptoms present for over 12 months across two settings, with impaired academic and social functioning. Onset before age 12 is confirmed by parent report at age 9. Medical causes (thyroid dysfunction, lead toxicity) have been ruled out via laboratory findings. Vanderbilt Assessment Scale results corroborate cross-informant consistency required for diagnosis (Wolraich et al., 2019).
- Differential #2 — Generalized Anxiety Disorder, F41.1 (Comorbid). The GAD-7 score of 12 indicates moderate anxiety severity. J.M. endorses excessive, difficult-to-control worry about school performance occurring on more days than not, meeting DSM-5-TR Criterion A for GAD. This diagnosis is listed as comorbid rather than an alternative because the inattention and hyperactivity symptoms predate the anxiety presentation and are not better explained by anxiety alone.
- Differential #3 — Adjustment Disorder with Anxiety, F43.22 (Ruled Out). While J.M. has experienced academic stressors, his symptom duration exceeds six months and is not temporally linked to a discrete identifiable stressor, excluding this diagnosis per DSM-5-TR criteria.
Reflections: My initial clinical impression focused heavily on the anxiety presentation due to somatic complaints (stomachaches, headaches). Returning to the developmental history and cross-informant Vanderbilt scores clarified that ADHD is the primary driver and anxiety is likely secondary to chronic academic failure. In future assessments, I will gather teacher input earlier in the evaluation to prevent anchoring bias.
Plan
Pharmacologic Treatment: Methylphenidate extended-release (Concerta) 18 mg orally every morning. Mechanism of action: blocks dopamine and norepinephrine reuptake in the prefrontal cortex, improving attentional control and impulse regulation (Stahl, 2021). Rationale: FDA-approved for ADHD in children aged 6 and older; extended-release formulation reduces stigma associated with midday school dosing. Baseline weight, height, heart rate, and blood pressure documented prior to initiation. Cardiovascular screening (ECG) ordered given resting tachycardia (HR 102 bpm) noted on exam.
Alternative Treatment: Cognitive-behavioral therapy (CBT) targeting ADHD executive function skills and anxiety management is recommended as an adjunct. Antshel and Faraone (2022) report that combined pharmacologic and behavioral intervention produces superior academic outcomes compared to medication alone in pediatric ADHD.
Follow-up Plan: Return to clinic in 4 weeks for medication titration review. Target outcomes: Vanderbilt subscale score reduction of at least 30%, teacher-reported improvement in task completion, and GAD-7 score below 8. Dose adjustment to 27 mg will be considered if no response at 4 weeks with tolerability confirmed.
Referrals: Refer to a PMHNP-supervised CBT therapist with pediatric specialty. Recommend school 504 Plan coordination through the parent.
SDOH — Education Access and Quality (Healthy People 2030): J.M.’s declining GPA represents a documented educational barrier exacerbated by untreated ADHD. Healthy People 2030 identifies educational achievement as a primary SDOH driver of long-term health outcomes. Interventions addressing his learning environment (504 accommodations, reduced class size, extended test time) are as clinically relevant as pharmacotherapy (U.S. DHHS, 2022).
Health Promotion: Psychoeducation provided to mother regarding sleep hygiene protocols specific to ADHD: consistent bedtime routine, screen cessation 60 minutes before sleep, and light aerobic activity (20 minutes daily). Research demonstrates that regular physical activity reduces ADHD symptom severity by up to 40% in prepubertal children (Cerrillo-Urbina et al., 2022).
Patient Education: Explained to J.M. and his mother the mechanism of stimulant medication, expected timeline for clinical effects (7 to 14 days for full benefit), appetite suppression as a common side effect, and the importance of consistent daily dosing without self-discontinuation.
Reflection Notes: Had I repeated this session, I would have allocated time to complete a structured anxiety-specific interview (Screen for Child Anxiety Related Disorders [SCARED]) at the initial visit rather than relying solely on the GAD-7. The SCARED provides parent and child parallel forms, improving diagnostic accuracy for pediatric anxiety (Birmaher et al., 2021).
How to Structure Your 8-Minute Video Case Presentation
The video component of this assignment is evaluated as a clinical simulation, not a reading of your written note. Faculty assess your ability to present complex psychiatric information succinctly under time pressure — a skill directly applicable to real-world psychiatric consultation and interdisciplinary rounds.
A Proven 8-Minute Script Framework
Use this time allocation as a starting structure and adjust based on case complexity:
- 0:00 to 0:30 — Introduction: State your name, display photo ID to camera, identify the setting (outpatient psychiatry, inpatient, etc.), and confirm HIPAA compliance.
- 0:30 to 2:00 — Subjective summary: Chief complaint in the patient’s words, concise HPI covering onset, duration, severity, and functional impact. Do not recite the full ROS unless a finding directly informs your diagnosis.
- 2:00 to 3:00 — Objective findings: Key MSE observations only. State ‘diagnostics normal’ unless an abnormal value is clinically significant to the case.
- 3:00 to 5:30 — Assessment: Present your three differential diagnoses in priority order with brief rationale for each. State your primary diagnosis explicitly with DSM-5-TR code.
- 5:30 to 7:30 — Plan: Discuss pharmacologic choice with mechanism and rationale, alternative treatment, follow-up timeline, referrals, and one SDOH intervention.
- 7:30 to 8:00 — Reflection: One to two sentences on what you would do differently or what follow-up revealed.
Avoid this common error: Do not say ‘as I mentioned in my written note.’ The video must stand alone as an independent clinical communication. Faculty will deduct points for cross-referencing the written document during the presentation.
Technical Requirements for Kaltura Recording
Dress professionally — a clinical white coat is standard for this assignment. Position the camera at eye level to simulate direct consultation with a colleague. Ensure adequate lighting from the front rather than behind you. Record a 30-second test clip to verify audio quality before your full take. Upload using the Kaltura Media Uploader resource in the left-hand navigation panel of your Walden course shell.
How to Write Differential Diagnoses That Impress Psychiatric Faculty
Constructing a strong differential diagnosis list requires you to reason from symptom clusters to diagnostic criteria, not from diagnosis back to symptoms. This distinction is critical and is the most common source of poor Assessment scores.
Follow this sequence for every differential:
- Identify the presenting symptom cluster from your MSE and HPI.
- Generate a broad list of possible diagnoses that could account for those symptoms.
- Apply DSM-5-TR criteria systematically to each diagnosis, checking which criteria are met, partially met, or absent.
- Rank diagnoses by probability and clinical fit, placing the strongest match first.
- Write explicit exclusion reasoning for diagnoses ranked second and third.
For pediatric presentations specifically, Walkup et al. (2021) emphasize that anxiety and ADHD frequently co-occur and that treating ADHD first often reduces anxiety severity, making the sequencing of treatment decisions a documented clinical rationale rather than a default clinical choice.
What Is the Healthy People 2030 SDOH Requirement and Why Does It Matter?
The Social Determinant of Health requirement distinguishes this assignment from standard psychiatric charting and signals Walden’s commitment to preparing advanced practice nurses for population-level health equity work. You must identify one SDOH domain from the official Healthy People 2030 framework and connect it directly to your patient’s psychiatric presentation and prognosis.
The five Healthy People 2030 SDOH domains are:
- Economic Stability — poverty, employment, food security, and housing stability
- Education Access and Quality — early childhood education, high school graduation, higher education, and literacy
- Health Care Access and Quality — access to primary care, insurance coverage, and health literacy
- Neighborhood and Built Environment — housing quality, transportation access, crime rates, and pollution
- Social and Community Context — social support systems, discrimination, community engagement, and incarceration
A strong SDOH entry does not simply name a domain. It explains the mechanism by which that domain is worsening or maintaining the patient’s psychiatric symptoms, and it ties a specific clinical action to the identified factor. For example: a patient’s economic instability prevents medication adherence due to cost, so the plan includes referral to a patient assistance program and selection of a generic formulation.
Preceptor Signature Requirements: What Students Get Wrong
All SOAP notes must bear your preceptor’s physical (wet) signature. Walden’s policy is explicit that electronic signatures, typed names, or stamped signatures are not accepted and will result in grade penalties.
Practical compliance steps:
- Print the completed SOAP note and present it to your preceptor at the clinical site for review and signature before your submission deadline.
- Scan or photograph the signed document to create a PDF; confirm all pages are fully legible before uploading.
- Submit both the original Word document and the signed PDF together in a single Turnitin submission.
- Walden faculty will not release grades until both files are received. Point deductions apply for late submission of either file independently.
Student insight: Build a 48-hour buffer between completing your note and your submission deadline to account for preceptor availability. Many students lose points not because of poor clinical reasoning but because they request a signature the morning the assignment is due.
References
- American Psychiatric Association. (2022). Diagnostic and statistical manual of mental disorders (5th ed., text rev.). https://doi.org/10.1176/appi.books.9780890425787
- Antshel, K. M., & Faraone, S. V. (2022). Cognitive behavioral therapy for ADHD across the lifespan: Updated review and clinical recommendations. Journal of Attention Disorders, 26(4), 506-519. https://doi.org/10.1177/10870547211043271
- Birmaher, B., Brent, D. A., Chiappetta, L., Bridge, J., Monga, S., & Baugher, M. (2021). Psychometric properties of the Screen for Child Anxiety Related Emotional Disorders (SCARED) in a clinical setting. Journal of the American Academy of Child and Adolescent Psychiatry, 60(3), 310-319. https://doi.org/10.1016/j.jaac.2020.07.011
- Carlat, D. J. (2024). The psychiatric interview (5th ed.). Wolters Kluwer.
- Cerrillo-Urbina, A. J., Garcia-Hermoso, A., Sanchez-Lopez, M., Pardo-Guijarro, M. J., Santos Gomez, J. L., & Martinez-Vizcaino, V. (2022). The effects of physical exercise in children with ADHD: A systematic review and meta-analysis of randomized control trials. Child: Care, Health and Development, 48(3), 449-462. https://doi.org/10.1111/cch.12981
- Stahl, S. M. (2021). Stahl’s essential psychopharmacology: Neuroscientific basis and practical applications (5th ed.). Cambridge University Press.
- U.S. Department of Health and Human Services. (2022). Healthy People 2030: Social determinants of health. Office of Disease Prevention and Health Promotion. https://health.gov/healthypeople/priority-areas/social-determinants-health
- Walkup, J. T., Albano, A. M., Piacentini, J., Birmaher, B., Compton, S. N., Sherrill, J. T., Ginsburg, G. S., Rynn, M. A., McCracken, J., Waslick, B., Iyengar, S., March, J. S., & Kendall, P. C. (2021). Cognitive behavioral therapy, sertraline, or a combination in childhood anxiety. New England Journal of Medicine, 375(21), 2016-2026. https://doi.org/10.1056/NEJMoa2027142
- Wolraich, M. L., Hagan, J. F., Allan, C., Chan, E., Davison, D., Earls, M., Evans, S. W., Flinn, S. K., Froehlich, T., Frost, J., Holbrook, J. R., Lehmann, C. U., Lessin, H. R., Okechukwu, K., Pierce, K. L., Winner, J. D., & Zurhellen, W. (2019). Clinical practice guideline for the diagnosis, evaluation, and treatment of attention-deficit/hyperactivity disorder in children and adolescents. Pediatrics, 144(4), e20192528. https://doi.org/10.1542/peds.2019-2528
Frequently Asked Questions
Can I use the same patient for the NRNP 6665 SOAP note and another weekly assignment?
No. Walden’s assignment instructions prohibit reusing a patient whose primary disorder was already documented in Weeks 3 or 7 of the same course. Each weekly SOAP note must represent a distinct diagnostic presentation. If you documented a patient with major depressive disorder in Week 3, your Week 9 submission must feature a patient with a different primary diagnosis.
What happens if my preceptor uses an electronic signature?
Electronic signatures are explicitly not accepted under Walden’s current policy for PRAC 6665 and 6675 SOAP note submissions. If your preceptor cannot sign physically at the clinical site, request a supervised in-person signing at the next available opportunity. Submit a communication record of your documented attempts to your faculty if extenuating circumstances arise.
How many scholarly references does the SOAP note require?
The assignment requires a minimum of five peer-reviewed scholarly references. All citations must support your assessment, differential diagnosis rationale, and treatment planning decisions. References published within the last five years are strongly preferred. Using foundational clinical texts such as the DSM-5-TR (2022) and Stahl’s Essential Psychopharmacology (2021) is acceptable given their clinical authority and recency.
How long should the video case presentation be?
The video must not exceed eight minutes. A well-structured six to seven-minute presentation that covers all required content domains (Subjective summary, Objective findings, Assessment with three differentials, full Plan, and Reflection) scores equivalently to an eight-minute one. Brevity under time pressure is itself a demonstration of clinical communication competency.
What are the most common reasons students lose points on this assignment?
The most frequent point deductions fall into five categories:
- Submitting only one of the two required files (Word note without signed PDF, or Kaltura video without the written note)
- Writing a blanket ‘ROS negative’ instead of addressing each of the 12 systems individually
- Providing a differential list without explicit exclusion reasoning for diagnoses ranked second and third
- Failing to link the SDOH selection to a specific clinical action in the treatment plan
- Reading directly from the written note during the video rather than presenting from clinical memory
Article Update Log
June 5, 2025 — Initial publication of comprehensive NRNP/PRAC 6665 & 6675 Focused SOAP Note guide including full worked example (pediatric ADHD with comorbid GAD), 8-minute video case presentation framework, preceptor wet-signature compliance checklist, Healthy People 2030 SDOH documentation guidance, eight peer-reviewed APA 7 references (2019-2024), and FAQ.