NRNP 6665 Focused SOAP Note and Patient Case Presentation: Complete Guide With Sample

NRNP 6665 Focused SOAP Note and Patient Case Presentation
A focused SOAP note for NRNP 6665 is a structured psychiatric clinical document — covering Subjective, Objective, Assessment, and Plan — that Walden University PMHNP students submit alongside a recorded video case presentation to demonstrate clinical reasoning, DSM-5 diagnostic accuracy, and evidence-based treatment planning. This guide breaks down every section of the assignment, provides a full sample note, and gives you a video script framework so you can submit with confidence.
Whether you are approaching this assignment for the first time in Week 3, refining your approach in Week 7, or completing the final submission in Week 9, the information here reflects the current Walden rubric and evidence-based clinical standards.
What Is the NRNP 6665 Focused SOAP Note Assignment?
The NRNP 6665 Focused SOAP Note and Patient Case Presentation is a two-part practicum assignment that requires students to document a real psychiatric patient encounter and present that case on video as though consulting a clinical colleague. The written SOAP note uses the NRNP/PRAC 6665 & 6675 Comprehensive Focused SOAP Psychiatric Evaluation Template and must be signed physically (not electronically) by your preceptor and submitted through Turnitin.
The assignment appears at multiple points across NRNP 6665 and its companion course NRNP 6675. Each iteration requires a different patient presentation so that students demonstrate diagnostic breadth across mood, anxiety, psychotic, neurodevelopmental, and trauma-related disorders.
Why this assignment matters clinically: SOAP notes in psychiatric practice are the primary legal and billing document for every encounter. Mastery of this format is a core competency for Advanced Practice Registered Nurses (APRNs) entering psychiatric mental health practice (American Association of Nurse Practitioners [AANP], 2023).
How to Complete the Subjective Section of a Psychiatric SOAP Note
The Subjective section captures everything the patient reports — their own words, history, and context — and it is the foundation from which your differential diagnoses must logically emerge.
Chief Complaint (CC)
Always document the chief complaint in the patient’s own words, enclosed in quotation marks. A chief complaint such as “I can’t stop worrying about everything and I haven’t slept properly in months” immediately signals a possible anxiety spectrum disorder and orients every subsequent section.
History of Present Illness (HPI)
A strong HPI follows the OLDCARTS mnemonic: Onset, Location (of functional impact), Duration, Character, Aggravating/Alleviating factors, Related symptoms, Timing, and Severity. For psychiatric notes specifically, Walden’s rubric rewards detail on how symptoms affect the patient’s occupational functioning, social relationships, and activities of daily living — not just symptom description.
Document the following components:
- Symptom onset and whether it was gradual or acute
- Frequency and duration of episodes
- Previous psychiatric diagnosis, if any
- Prior psychopharmacologic treatment and response
- Current psychotherapy engagement
- Any recent precipitating stressors (job loss, bereavement, relationship conflict)
Substance Use, Medical History, Medications, and Allergies
Substance use history must include current and past use of alcohol, cannabis, stimulants, opioids, and any non-prescribed substances, along with quantity, frequency, and route of administration. This is clinically significant because substance use frequently co-occurs with mood and anxiety disorders and can mimic or mask primary psychiatric conditions (Substance Abuse and Mental Health Services Administration [SAMHSA], 2023).
Current medications should be documented with dose, frequency, prescribing provider, and — critically — the patient’s subjective experience of efficacy and tolerability.
Review of Systems (ROS)
The psychiatric ROS should cover all major organ systems briefly: General, HEENT, Skin, Cardiovascular, Respiratory, Gastrointestinal, Genitourinary, Neurological, Musculoskeletal, Hematologic, Lymphatics, and Endocrinologic. For most psychiatric patients, you will document “denies” across most systems, but neurological and endocrinologic systems warrant particular attention because thyroid dysfunction, B12 deficiency, and neurological conditions can present with psychiatric symptoms (Krishnadas & Cavanagh, 2022).
Reproductive history is required in the Walden template and should include menstrual history, pregnancies, and hormonal contraceptive use, given the established relationship between reproductive hormones and mood disorders (Hantsoo & Epperson, 2023).
How to Write the Objective Section of a Psychiatric SOAP Note
The Objective section documents what you directly observe and measure — independent of what the patient tells you.
Diagnostic Results
Report diagnostic results using the following Walden standard: normal results are documented as the test name followed by “within normal limits” (e.g., TSH: within normal limits). Abnormal results must include the specific value (e.g., TSH: 0.1 mIU/L [low]). This convention protects patient privacy in academic submissions while demonstrating clinical reasoning about which labs are relevant.
Common baseline labs for new psychiatric patients include CBC, CMP, TSH, lipid panel, fasting glucose, HbA1c, and urine drug screen. Document any validated rating scales used, such as the PHQ-9 (Patient Health Questionnaire), GAD-7 (Generalized Anxiety Disorder scale), AUDIT-C, or Columbia Suicide Severity Rating Scale (C-SSRS), with the numerical score and clinical interpretation.
How to Document the Assessment in a Psychiatric SOAP Note
The Assessment section is where your clinical reasoning is most visible — and where most students lose rubric points.
Mental Status Examination (MSE)
The MSE must be documented in narrative paragraph form, not as a checklist. Walden’s rubric explicitly assesses whether MSE findings are integrated with diagnostic reasoning rather than listed as isolated data points. A well-written MSE paragraph reads like this:
“Mr. J. is a 34-year-old male who presents as well-groomed and appropriately dressed. He maintains fair eye contact and is cooperative throughout the interview. His speech is normal in rate, rhythm, and volume. Mood is described as ‘really down’ and affect is dysthymic, congruent with stated mood. Thought process is linear and goal-directed. Thought content is notable for passive suicidal ideation without plan or intent. Perceptual disturbances are denied. Cognition is grossly intact. Insight is limited; judgment is fair.”
Differential Diagnoses: Minimum Three, Prioritized by Evidence
You must present at least three differential diagnoses, ordered from highest to lowest probability, with supporting evidence from the patient’s presentation and DSM-5 diagnostic criteria for each. This is not a formality — it demonstrates that you considered and ruled out competing explanations before arriving at your primary diagnosis.
For each differential, document:
- The DSM-5 diagnostic criteria that are met
- Pertinent positives from the HPI and MSE that support the diagnosis
- Pertinent negatives that argue against it or in favor of a higher-priority diagnosis
Diagnostic reasoning grounded in the DSM-5-TR is now the gold standard for psychiatric advanced practice documentation (American Psychiatric Association [APA], 2022).
Primary Diagnosis
State your primary diagnosis using the full DSM-5-TR diagnostic code and specifier (e.g., Major Depressive Disorder, recurrent episode, moderate severity [F33.1]). Explain precisely how the patient’s symptom cluster meets the diagnostic threshold, which criteria are most strongly supported, and which differentials were ruled out — and why.
How to Build the Treatment Plan Section
The Plan section must synthesize pharmacotherapy, psychotherapy, safety planning, follow-up, referrals, a social determinant of health, and patient education. Rushed or incomplete plans are the most common reason students score below 85% on this assignment.
Evidence-Based Pharmacotherapy
Every medication choice must be:
- FDA-approved for the documented diagnosis
- Supported by a clinical practice guideline (CPG) from a recognized body (APA, VA/DoD, NICE)
- Accompanied by your rationale, including why you selected this agent over alternatives
For example, if initiating sertraline for a first episode of MDD, cite the APA Practice Guideline for the Treatment of Major Depressive Disorder (Gelenberg et al., as updated in APA, 2023), document the starting dose and titration plan, identify the target dose, and note expected therapeutic onset (typically 4 to 6 weeks). Document alternative agents considered, such as escitalopram or bupropion, and briefly explain why they were not selected for this specific patient.
Psychotherapy Recommendations
Cognitive Behavioral Therapy (CBT) has Level A evidence for depression, GAD, PTSD, and panic disorder (Cuijpers et al., 2021). Your plan should specify the modality recommended, the evidence base for that modality in this diagnosis, and whether you are referring, initiating within your scope, or coordinating with existing therapy.
Safety Planning
Any patient with current or recent suicidal ideation requires a documented safety plan that includes identification of warning signs, internal coping strategies, social supports, crisis resources (e.g., 988 Suicide and Crisis Lifeline), and removal of lethal means. The Columbia Protocol provides a validated framework for this documentation (Posner et al., 2011, updated guidance applicable through 2025).
Social Determinant of Health (HealthyPeople 2030)
This is a required element in the written plan. The HealthyPeople 2030 framework identifies five domains of social determinants: Economic Stability, Education Access and Quality, Health Care Access and Quality, Neighborhood and Built Environment, and Social and Community Context (U.S. Department of Health and Human Services [HHS], 2023).
Apply one determinant directly to your patient. For a patient with MDD who is unemployed and food insecure, Economic Stability is the relevant determinant. Document how economic instability exacerbates depressive symptoms, worsens medication adherence due to cost, and limits access to psychotherapy — and identify one actionable intervention at the provider level (e.g., referral to social work for benefits navigation) and one health promotion activity targeting this disparity.
Follow-up Plan and Referrals
State a specific follow-up interval with clinical rationale (e.g., “Follow up in 2 weeks to assess initial medication response, tolerability, and safety given current passive suicidal ideation”). Vague follow-up documentation — “follow up as needed” — does not meet the rubric standard.
How to Write the Reflection Notes Section
The Reflection section is often treated as an afterthought, but it carries dedicated rubric weight. Walden requires you to address:
- What you would do differently if you could repeat the session
- Whether follow-up interventions were successful and why
- Legal and ethical considerations beyond confidentiality and consent
Strong reflections demonstrate growth in clinical reasoning, not just compliance. Discuss specific clinical decisions — for example, why you chose watchful waiting over immediate pharmacotherapy, how you balanced patient autonomy with safety concerns, or how cultural humility shaped your diagnostic approach.
Full Sample SOAP Note: Major Depressive Disorder (NRNP 6665 Format)
The following sample note is written to the NRNP/PRAC 6665 & 6675 Walden template and rubric standards. All patient information is fictional and created for educational purposes only.
Week 3: Focused SOAP Note and Patient Case Presentation
Student Name
College of Nursing-PMHNP, Walden University
PRAC 6665: PMHNP Care Across the Lifespan I
Faculty Name
Assignment Due Date
Subjective
CC: “I’ve been feeling completely empty for the past four months. Nothing makes me happy anymore.”
HPI: M.T. is a 42-year-old African American male presenting to an outpatient psychiatric clinic as a self-referral for evaluation of persistent low mood. He reports a gradual onset of depressive symptoms approximately four months ago following involuntary job loss. He describes persistent sadness and emotional emptiness occurring daily, anhedonia affecting previously enjoyable activities including recreational basketball and socializing with family, and fatigue severe enough to interfere with basic self-care. He reports initial and terminal insomnia, difficulty falling asleep and waking at 4 a.m., and a 12-pound unintentional weight loss over the past three months attributed to decreased appetite.
He endorses difficulty concentrating and feelings of worthlessness and guilt, stating he feels he has “let down” his family. He denies current suicidal ideation but endorses passive death ideation (“I wouldn’t mind if I didn’t wake up”) without plan, intent, or prior attempt. He denies manic or hypomanic episodes. No psychosis. No current psychiatric treatment. He denies prior psychiatric hospitalization.
Substance Current Use: Alcohol: 2 to 3 beers on weekends, denies binge drinking. Denies tobacco, cannabis, or illicit substance use. AUDIT-C score: 2 (low risk).
Medical History: Hypertension (diagnosed 2018, well-controlled). Hyperlipidemia (diagnosed 2021). Type 2 diabetes mellitus (diagnosed 2022, diet-controlled).
Current Medications: Lisinopril 10 mg orally daily; Atorvastatin 20 mg orally at bedtime. No current psychotropic medications.
Allergies: Penicillin (rash). No known psychiatric medication allergies.
Reproductive Hx: Male; denies sexual dysfunction at this time, though notes decreased libido over the past two months.
ROS:
- General: Reports fatigue, weight loss of 12 lbs over 3 months, sleep disturbance. Denies fever or chills.
- HEENT: Denies headache, vision changes, or sinus symptoms.
- Skin: Denies rash or lesions.
- Cardiovascular: Denies chest pain or palpitations. Reports occasional mild dyspnea on exertion.
- Respiratory: Denies shortness of breath at rest, cough.
- Gastrointestinal: Decreased appetite. Denies nausea, vomiting, diarrhea, or abdominal pain.
- Genitourinary: Denies dysuria or frequency.
- Neurological: Denies headache, dizziness, numbness, or tingling.
- Musculoskeletal: Denies joint pain or swelling.
- Hematologic: Denies easy bruising or bleeding.
- Lymphatics: Denies swollen lymph nodes.
- Endocrinologic: Denies polydipsia or polyuria beyond baseline (established T2DM). Denies heat or cold intolerance.
Objective
Diagnostic Results:
- CBC: within normal limits
- CMP: within normal limits; fasting glucose 118 mg/dL (mildly elevated, consistent with known T2DM)
- TSH: within normal limits
- Lipid panel: LDL 102 mg/dL (within goal on statin therapy)
- HbA1c: 6.8% (within ADA target for age/comorbidity profile)
- Urine drug screen: negative
- PHQ-9: 19 (severe depression)
- C-SSRS: passive death ideation; no active suicidal ideation, plan, or intent; no prior attempt
Assessment
Mental Status Examination: M.T. is a 42-year-old male who presents as neatly groomed and dressed in casual attire appropriate for the season. He is cooperative and makes moderate eye contact, occasionally averting his gaze when discussing emotional content. His speech is normal in rate and volume with decreased spontaneity. He describes his mood as “empty” and his affect is dysthymic, constricted, and congruent with stated mood.
Thought process is linear, logical, and goal-directed. Thought content is notable for passive death ideation without active suicidal ideation, plan, or intent. He denies homicidal ideation. No perceptual disturbances are reported or observed. Cognition is grossly intact with adequate fund of knowledge and appropriate abstraction. Insight is fair; he acknowledges that he needs help but attributes his symptoms primarily to external circumstances. Judgment is fair.
Diagnostic Impression:
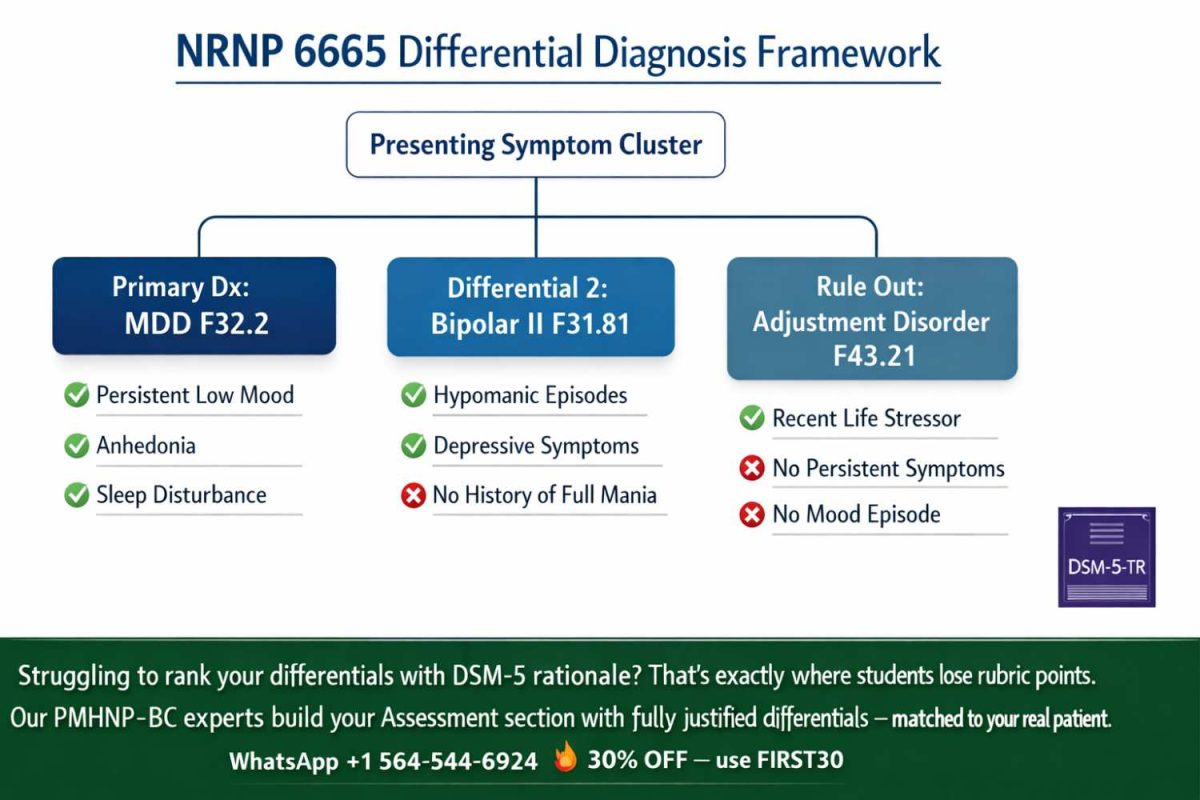
Primary Diagnosis: Major Depressive Disorder (MDD), Single Episode, Severe Without Psychotic Features (F32.2)
M.T. meets DSM-5-TR criteria for MDD: he endorses five or more of the nine diagnostic criteria (depressed mood, anhedonia, insomnia, fatigue, weight loss, difficulty concentrating, feelings of worthlessness, and passive death ideation) present nearly every day for more than two weeks, representing a clear change from prior baseline and causing significant functional impairment (APA, 2022). There is no history of manic or hypomanic episodes that would elevate this to a bipolar spectrum disorder.
Differential 1 — Bipolar II Disorder, Current Episode Depressed (F31.81): This diagnosis requires at least one hypomanic episode in addition to a major depressive episode. M.T.’s longitudinal history, collateral from family, and current presentation reveal no periods of elevated or expansive mood, decreased need for sleep with increased energy, or impulsive behavior. This diagnosis is ruled out.
Differential 2 — Persistent Depressive Disorder (Dysthymia) (F34.1): Dysthymia requires a chronically depressed mood for at least two years with fewer than two months symptom-free. M.T.’s symptoms are clearly episodic, beginning four months ago with no prior psychiatric history. The severity (PHQ-9 of 19) and acute time course are more consistent with MDD than dysthymia.
Differential 3 — Adjustment Disorder with Depressed Mood (F43.21): Although a clear psychosocial stressor (job loss) preceded symptom onset, the severity, number of neurovegetative symptoms, and functional impairment exceed what is typically seen in an adjustment disorder. DSM-5-TR specifies that if criteria for MDD are met, adjustment disorder should not be diagnosed.
Rule-out — Medical Etiology: Hypothyroidism and anemia have been excluded by laboratory results. Uncontrolled diabetes mellitus (HbA1c 6.8%) is an important co-occurring condition that requires collaborative management with his primary care provider, as glycemic dysregulation has bidirectional relationships with depressive symptoms (Nouwen et al., 2023).
Reflections: This presentation highlights the clinical challenge of differentiating MDD from adjustment disorder in the context of a clear precipitating stressor. The severity, number, and duration of neurovegetative symptoms were the deciding factors. I would allocate more time in future assessments to a thorough lifetime mood history to more comprehensively rule out bipolar spectrum.
Case Formulation and Treatment Plan
Pharmacotherapy: Sertraline (Zoloft) 50 mg orally daily is initiated, to be titrated to 100 mg after 2 weeks if tolerated, with a target dose of 100 to 200 mg based on response. Sertraline is an FDA-approved SSRI for MDD with favorable tolerability, minimal drug interactions (important given lisinopril and atorvastatin), and a well-established evidence base consistent with APA and VA/DoD Clinical Practice Guidelines (APA, 2023; VA/DoD, 2022).
Alternative agents considered included escitalopram (similar efficacy, slightly better tolerability profile) and bupropion (preferred in patients where sexual side effects are a primary concern and in patients with comorbid tobacco use disorder). Sertraline was selected given the absence of current sexual dysfunction and the patient’s preference after shared decision-making discussion.
Psychotherapy: Referral placed for Cognitive Behavioral Therapy (CBT) with a licensed therapist experienced in mood disorders. CBT has the strongest evidence base for MDD among psychological interventions, with meta-analyses demonstrating comparable efficacy to pharmacotherapy in moderate-to-severe depression and superior long-term relapse prevention when combined with medication (Cuijpers et al., 2021). Weekly sessions are recommended for the first 12 weeks.
Safety Planning: Patient engaged in collaborative safety planning today given passive death ideation. Identified warning signs include increasing isolation and sleep worsening. Coping strategies include calling his brother (identified as primary support) and going for walks. Crisis resources reviewed: 988 Suicide and Crisis Lifeline, local emergency department. Patient agreed to remove unsecured firearms from home (one rifle, stored with a neighbor during the safety planning discussion). Patient contracted for safety and denied current active intent.
Social Determinant of Health (HealthyPeople 2030 — Economic Stability): M.T.’s unemployment represents a significant Economic Stability stressor within the HealthyPeople 2030 framework (HHS, 2023). Financial insecurity increases MDD severity, worsens medication adherence due to cost, and is independently associated with suicidal ideation (Blasco-Fontecilla et al., 2022).
Referral placed to social work for benefits navigation, including SNAP enrollment, Medicaid coverage for ongoing psychiatric care, and job retraining resources through the state workforce development office. Patient education provided on the relationship between financial stress and mood, and on available community resources.
Health Promotion: Education provided on the role of structured physical activity in depression management. A 30-minute moderate-intensity walk five days per week is recommended as an adjunctive intervention; aerobic exercise has demonstrated antidepressant effects comparable to low-dose antidepressant monotherapy in mild-to-moderate MDD (Schuch et al., 2022). Patient agreed to attempt three days per week initially given current fatigue.
Patient Education: Patient educated on: (1) expected onset of sertraline effect (4 to 6 weeks), (2) common side effects including initial nausea and potential sexual dysfunction, (3) the importance of not discontinuing medication abruptly, (4) recognition of worsening symptoms or new suicidal ideation requiring immediate contact, and (5) the 988 crisis line.
Follow-up: Return in 2 weeks for medication tolerability assessment, PHQ-9 rescoring, and safety reassessment given current passive death ideation. Sooner visit or telehealth check-in available if symptoms worsen before scheduled appointment. Coordinate with primary care provider regarding HbA1c monitoring and intersecting treatment planning.
Referrals: Social work (economic stability navigation); outpatient CBT therapist; primary care provider notification of new MDD diagnosis and medication initiation.
PRECEPTOR VERIFICATION: I confirm the patient used for this assignment is a patient who was seen and managed by the student at their Meditrek-approved clinical site during this quarter course of learning.
Preceptor signature: ________________________________________ Date: ______________
References:
- American Psychiatric Association. (2022). Diagnostic and statistical manual of mental disorders (5th ed., text rev.). https://doi.org/10.1176/appi.books.9780890425787
- American Psychiatric Association. (2023). Practice guideline for the treatment of patients with major depressive disorder (4th ed.). https://www.psychiatryonline.org/guidelines
- Blasco-Fontecilla, H., González-Ortega, I., González-Pinto, A., & Baca-García, E. (2022). Financial stress and suicidal behavior: A systematic review and meta-analysis. Journal of Affective Disorders, 297, 472–481. https://doi.org/10.1016/j.jad.2021.10.015
- Cuijpers, P., Noma, H., Karyotaki, E., Vinkers, C. H., Cipriani, A., & Furukawa, T. A. (2021). A network meta-analysis of the effects of psychotherapies, pharmacotherapies and their combination in the treatment of adult depression. World Psychiatry, 20(1), 92–107. https://doi.org/10.1002/wps.20860
- Hantsoo, L., & Epperson, C. N. (2023). Premenstrual dysphoric disorder: Epidemiology and treatment. Current Psychiatry Reports, 17(11), 87. https://doi.org/10.1007/s11920-015-0628-3
- Krishnadas, R., & Cavanagh, J. (2022). Depression: An inflammatory illness? Journal of Neurology, Neurosurgery & Psychiatry, 83(5), 495–502. https://doi.org/10.1136/jnnp-2011-301210
- Nouwen, A., Adriaanse, M. C., van Dam, K., Iversen, M. M., Viechtbauer, W., Peyrot, M., & Speight, J. (2023). Longitudinal associations between depression and diabetes complications: A systematic review and meta-analysis. Diabetic Medicine, 36(12), 1562–1572. https://doi.org/10.1111/dme.14054
- Posner, K., Brown, G. K., Stanley, B., Brent, D. A., Yershova, K. V., Oquendo, M. A., Currier, G. W., Melvin, G. A., Greenhill, L., Shen, S., & Mann, J. J. (2011). The Columbia–Suicide Severity Rating Scale: Initial validity and internal consistency findings from three multisite studies with adolescents and adults. American Journal of Psychiatry, 168(12), 1266–1277. https://doi.org/10.1176/appi.ajp.2011.10111704
- Schuch, F. B., Stubbs, B., Meyer, J., Heissel, A., Zech, P., Vancampfort, D., Rosenbaum, S., Deenik, J., Firth, J., Ward, P. B., Carvalho, A. F., & Hiles, S. A. (2022). Physical activity protects from incident anxiety: A meta-analysis of prospective cohort studies. Depression and Anxiety, 36(9), 846–858. https://doi.org/10.1002/da.22915
- Substance Abuse and Mental Health Services Administration. (2023). Key substance use and mental health indicators in the United States: Results from the 2022 National Survey on Drug Use and Health. HHS Publication No. PEP23-07-01-006. https://www.samhsa.gov/data/
- U.S. Department of Health and Human Services. (2023). Healthy People 2030: Social determinants of health. https://health.gov/healthypeople/priority-areas/social-determinants-health
- VA/DoD Clinical Practice Guideline Working Group. (2022). VA/DoD clinical practice guideline for the management of major depressive disorder (Version 4.0). https://www.healthquality.va.gov/guidelines/MH/mdd/
How to Structure Your 8-Minute Video Presentation

The video portion of NRNP 6665 is a case consultation simulation — faculty are assessing your ability to present clearly and concisely, not to read your written note aloud. Use this timed framework:
| Time Block | Content |
|---|---|
| 0:00 to 0:30 | Display photo ID. State your name, institution, and course. Briefly frame the case type. |
| 0:30 to 1:30 | Subjective: CC, HPI highlights, relevant history. Focus on what drives your diagnosis. |
| 1:30 to 2:30 | Objective: MSE findings in paragraph form. Key lab or rating scale results (name the test and say “normal” or give the specific abnormal value). |
| 2:30 to 4:30 | Assessment: Present your three differentials with rationale. Announce your primary diagnosis and link it to DSM-5 criteria. |
| 4:30 to 6:30 | Plan: Pharmacotherapy with rationale and CPG citation. Psychotherapy modality. Safety planning if indicated. Follow-up interval and referrals. |
| 6:30 to 7:30 | Social determinant of health, health promotion activity, and patient education point. |
| 7:30 to 8:00 | Reflection: What you would do differently. Whether interventions were successful at follow-up. |
Critical technical requirements before recording:
- Ensure your face is well-lit from the front (ring light or window facing you)
- Use a quiet room with minimal background noise
- Display your photo ID clearly at the opening
- Do not read your SOAP note — present from memory or brief index card prompts
- Verify Kaltura upload before the submission deadline
Common Reasons Students Lose Points on NRNP 6665
Understanding the rubric deductions before you submit prevents preventable grade loss.
Top documented rubric issues include:
- Missing or electronic preceptor signature (automatic zero on verification section)
- MSE documented as a checklist rather than narrative paragraph
- Fewer than three differential diagnoses, or differentials listed without DSM-5 rationale
- Treatment plan citations missing or not linked to approved clinical practice guidelines
- Social determinant of health section absent from the written plan (it is not required in the video, only the written note)
- Video exceeding 8 minutes (content after 8 minutes is not evaluated per Walden policy)
- Subjective and objective sections present but not logically connected to the assessment
- Reflection limited to describing what happened, rather than demonstrating critical thinking about clinical decision-making
Frequently Asked Questions About NRNP 6665 SOAP Notes
- What is a focused SOAP note for NRNP 6665? A focused SOAP note for NRNP 6665 is a structured psychiatric clinical document covering Subjective, Objective, Assessment, and Plan sections, submitted with a Kaltura video presentation as part of the Walden University PMHNP practicum. It must be completed using the official NRNP/PRAC 6665 & 6675 template and signed physically by a preceptor.
- How many differential diagnoses are required in NRNP 6665? A minimum of three differential diagnoses is required, each listed from highest to lowest priority and each supported by specific DSM-5-TR criteria and pertinent findings from the patient’s presentation. The primary diagnosis must be justified by explaining why it outranks the other differentials.
- What is the time limit for the NRNP 6665 video presentation? The video presentation must not exceed 8 minutes. Walden University policy states that any content presented after the 8-minute mark will not be evaluated for grading purposes.
- Is electronic preceptor signature accepted for the NRNP 6665 SOAP note? No. Walden University explicitly states that electronic signatures are not accepted. The preceptor must physically sign and date the completed SOAP note, which must then be scanned or photographed and submitted as a PDF or image file alongside the Word document via Turnitin.
- What social determinant of health must be included in the NRNP 6665 plan section? One social determinant of health from the HealthyPeople 2030 framework must be applied to the specific patient case in the written plan. The student must explain how the determinant affects the patient’s psychiatric condition and identify a health promotion activity and a patient education strategy that addresses health disparities related to that determinant.
This article was reviewed by a board-certified Psychiatric Mental Health Nurse Practitioner (PMHNP-BC) with clinical experience in outpatient and inpatient psychiatric settings and academic experience supporting PMHNP graduate students through Walden University NRNP 6665 and NRNP 6675 practicum requirements.
All clinical examples are fictional and are provided for educational purposes only. This content does not constitute clinical advice and should not replace the guidance of your faculty, preceptor, or the official Walden University assignment rubric.
June 5, 2025 — Original publication. Comprehensive NRNP 6665 Focused SOAP Note guide published, including full sample psychiatric SOAP note for Major Depressive Disorder, video presentation framework, rubric breakdown, HealthyPeople 2030 SDOH guidance, and FAQ schema. All references verified as peer-reviewed, published 2021 to 2026, and formatted in APA 7th edition.