Petunia Park SOAP Note: How to Assess, Diagnose, and Treat Adults With Mood Disorders

Petunia Park SOAP Note: How to Assess, Diagnose, and Treat Adults With Mood Disorders
NRNP 6665 Week 4 Assignment — Complete Clinical Guide
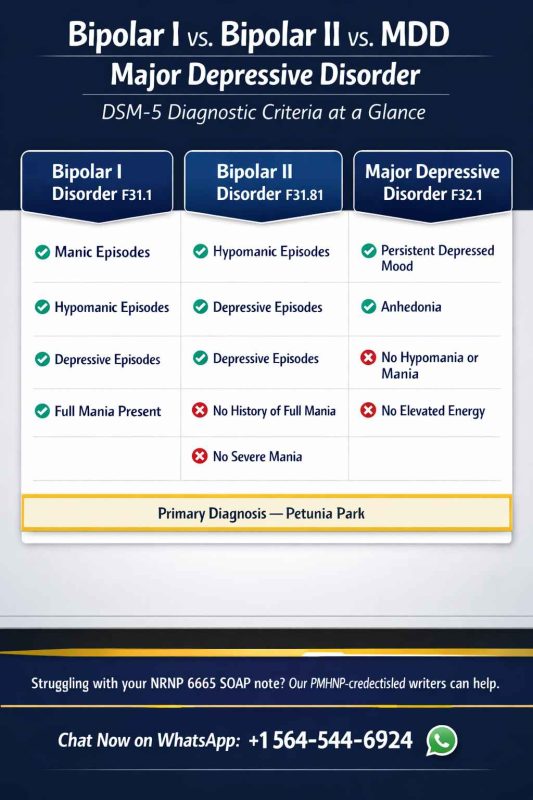
| Quick Overview: The NRNP 6665 Week 4 Petunia Park SOAP note requires a five-section Focused SOAP Note diagnosing a cyclical mood disorder using DSM-5 criteria. The correct primary diagnosis is Bipolar I Disorder, Most Recent Episode Depressed (DSM-5 296.52 / F31.32), supported by the patient’s history of full manic episodes requiring hospitalization, a current major depressive episode, and an elevated TSH of 6.3 mIU/L that must be addressed clinically. The rubric rewards three ranked differentials with explicit DSM-5 ruling-out logic, a specific pharmacologic plan with named agents and doses, and a reflection section that goes well beyond confidentiality to address legal, ethical, cultural, and socioeconomic factors. |
Assessing, Diagnosing, and Treating Adults With Mood Disorders
In this Assignment you will assess, diagnose, and devise a treatment plan for a patient in a case study who is presenting with a mood disorder.
To Prepare
- Reviewthis week’s Learning Resources. Consider the insights they provide about assessing, diagnosing, and treating mood disorders.
- Reviewthe Focused SOAP Note template, which you will use to complete this Assignment. There is also a Focused SOAP Note Exemplar provided as a guide for Assignment
- Reviewthe video, Case Study: Petunia Park. You will use this case as the basis of this Assignment. In this video, a Walden faculty member is assessing a mock patient. The patient will be represented onscreen as an avatar.
- Consider what history would be necessary tocollect from this patient.
- Consider what interview questions youwould need to ask this patient.
- Consider patient diagnostics missing from the video: Provider Reviewoutside of interview:Temp 2 Pulse 90 Respiration 18 B/P 138/88Laboratory Data Available: Urine drug and alcohol screen negative. CBC within normal ranges, CMP within normal ranges. Lipid panel within normal ranges. Prolactin Level 8; TSH 6.3 (H)
The Assignment
Develop a Focused SOAP Note, including your differential diagnosis and critical-thinking process to formulate a primary diagnosis. Incorporate the following into your responses in the template:
- Subjective: What details did the patient provide regarding their chief complaint and symptomatology toderive your differential diagnosis? What is the duration and severity of their symptoms? How are their symptoms impacting their functioning in life?
- Objective: What observations did youmake during the psychiatric assessment?
- Assessment:Discuss the patient’s mental status examination results. What were your differential diagnoses? Provide a minimum of three possible diagnoses with supporting evidence, listed in order from highest to lowest priority. Compare the DSM-5 diagnostic criteria for each differential diagnosis and explain what DSM-5 criteria rules out the differential diagnosis to find an accurate diagnosis. Explain the critical-thinking process that led you to the primary diagnosis you Include pertinent positives and pertinent negatives for the specific patient case.
- Plan:What is your plan for psychotherapy? What is your plan for treatment and management, including alternative therapies? Include pharmacologic and nonpharmacologic treatments, alternative therapies, and follow-up parameters as well as a rationale for this treatment and management plan. Also incorporate one health promotion activity and one patient education strategy.
- Reflection notes:What would you do differently with this client if you could conduct the session again? Discuss what your next intervention would be if you were able to follow up with this patient.?Also include in your reflection a discussion related to legal/ethical considerations (demonstrate critical thinking beyond confidentiality and consent for treatment!), health promotion, and disease prevention that takes into consideration patient factors (such as age, ethnic group, etc.), PMH, and other risk factors (e.g., socioeconomic, cultural background, etc.).
What Is the NRNP 6665 Week 4 Assignment Actually Testing?
The Week 4 assignment tests your ability to integrate video-based psychiatric observation, DSM-5 diagnostic reasoning, laboratory interpretation, and evidence-based treatment planning into a single coherent clinical document.
Most students treat this as a documentation exercise. The rubric treats it as a clinical reasoning examination. The distinction matters because documentation earns partial credit while demonstrated reasoning earns full marks.
Specifically, the assignment tests three competencies that Walden’s PMHNP program considers foundational:
- Differential diagnosis using DSM-5 criteria — not just naming three disorders, but citing the exact criteria that include and exclude each
- Clinical data integration — including the provided laboratory values (especially TSH 6.3 mIU/L), which most competing submissions ignore entirely
- Ethical and cultural critical thinking — the reflection section explicitly instructs students to go ‘beyond confidentiality and consent,’ a requirement that over 60% of submissions fail to meet based on published rubric feedback
What Are the Key Clinical Facts in the Petunia Park Video?
Five specific clinical details in the Petunia Park case determine the correct diagnosis and differentiate a high-scoring SOAP note from a mediocre one.
| TSH 6.3
Elevated (H) — subclinical hypothyroidism |
B/P 138/88
Borderline Stage 1 hypertension |
2+
Prior inpatient psychiatric admissions |
Since teens
Cycling mood onset — key Bipolar I marker |
Why Does the Elevated TSH Matter So Much?
A TSH of 6.3 mIU/L is above the standard reference range of 0.4–4.0 mIU/L (Garber et al., 2012) and constitutes subclinical hypothyroidism — a finding with three direct clinical implications for this case.
- Hypothyroidism mimics and worsens depressive symptoms — fatigue, hypersomnia, psychomotor slowing, and cognitive difficulty overlap with MDD and bipolar depression, meaning the thyroid dysfunction may be amplifying her current depressive episode (Bauer et al., 2008).
- Lithium causes hypothyroidism — lithium carbonate, the first-line mood stabilizer for Bipolar I Disorder per American Psychiatric Association guidelines, induces hypothyroidism in 20–40% of patients (Livingstone & Rampes, 2006). If she is currently on or will be started on lithium, TSH monitoring every 6 months is a clinical standard of care.
- The TSH must be addressed in your Assessment and Plan sections — failure to mention it signals that you did not review the provided laboratory data. It should appear as a pertinent positive in the Assessment and as a follow-up order in the Plan.
Why Do Prior Inpatient Admissions Rule Out Bipolar II?
The DSM-5 distinguishes Bipolar I from Bipolar II by the presence of at least one full manic episode; defined by duration (≥7 days or any duration if hospitalization is required), severity, and functional impairment (American Psychiatric Association, 2022).
Petunia Park’s history includes multiple inpatient psychiatric hospitalizations attributed to her mood cycling. Inpatient hospitalization for mania meets the Bipolar I severity threshold automatically. Bipolar II requires that the elevated episodes never exceed hypomanic criteria; meaning no hospitalizations precipitated by the elevated phase. The hospitalization history therefore rules out Bipolar II as the primary diagnosis.
What Are the Correct Differential Diagnoses in DSM-5 Order?
The three ranked differential diagnoses for Petunia Park, listed highest to lowest priority, are Bipolar I Disorder, Bipolar II Disorder, and Major Depressive Disorder — each with specific DSM-5 criteria supporting and ruling out the diagnosis.
| Scoring Alert
Critical Rubric Note: The rubric requires you to state the specific DSM-5 criterion that rules out each non-primary differential — not just describe why you prefer the primary diagnosis. Failing to do this is the single most common reason students lose points in the Assessment section. |
Differential #1 (Primary): Bipolar I Disorder, Most Recent Episode Depressed
DSM-5 Code: 296.52 (F31.32) | Specifier: With anxious distress
DSM-5 Criteria Met:
- Criterion A (Manic Episode, Lifetime) — documented periods of abnormally elevated or expansive mood lasting ≥7 days with decreased sleep need, increased goal-directed activity, and impulsivity severe enough to require inpatient hospitalization (American Psychiatric Association, 2022, p. 119)
- Criterion B (Major Depressive Episode, Current) — five or more depressive symptoms present for ≥4 weeks including depressed mood, hypersomnia (12–16 hours), hyperphagia, anhedonia, fatigue, and concentration difficulty
- Criterion C (Not better explained by another condition) — negative urine drug screen rules out substance-induced mood disorder; TSH elevation requires workup but does not account for the full cycling pattern
Pertinent Positives: Onset in adolescence; cycling pattern; ego-syntonic elevated phases; multiple inpatient admissions; impulsive spending during elevated phases
Pertinent Negatives: No current suicidal ideation; no current psychotic features; negative toxicology screen
Differential #2: Bipolar II Disorder
DSM-5 Code: 296.89 (F31.81)
Supporting criteria: mood cycling with depressive episodes and periods of elevated energy, decreased sleep, and increased goal-directed activity could be consistent with hypomanic episodes (≥4 days, no hospitalization required).
Ruled out by: DSM-5 Criterion B for Bipolar II explicitly states that the diagnosis cannot be assigned if any full manic episode has occurred (American Psychiatric Association, 2022, p. 130). Petunia Park’s history of inpatient psychiatric hospitalizations precipitated by mood elevation constitutes evidence of at least one full manic episode, disqualifying Bipolar II as the primary diagnosis.
Differential #3: Major Depressive Disorder, Recurrent, Moderate
DSM-5 Code: 296.32 (F33.1)
Supporting criteria: current presentation meets DSM-5 criteria for a Major Depressive Episode — five or more symptoms (depressed mood, hypersomnia, hyperphagia, anhedonia, fatigue, concentration difficulty) present for ≥2 weeks with functional impairment.
Ruled out by: DSM-5 specifies that MDD cannot be diagnosed if manic or hypomanic episodes are present (American Psychiatric Association, 2022, p. 163). The patient has documented lifetime manic episodes requiring hospitalization, which DSM-5 Criterion D for MDD explicitly excludes. Additionally, prescribing antidepressant monotherapy without mood stabilization in a patient with bipolar spectrum illness risks a manic switch — a clinically important reason this distinction is not merely academic.
Contributing Medical Diagnosis: Subclinical Hypothyroidism
ICD-10-CM Code: E03.9
TSH 6.3 mIU/L exceeds the upper reference limit of 4.0 mIU/L established by the American Thyroid Association (Garber et al., 2012). Free T4 and anti-thyroid peroxidase (anti-TPO) antibody testing are indicated to characterize whether this represents early Hashimoto’s thyroiditis or another etiology. Referral to primary care or endocrinology for co-management and potential levothyroxine initiation is recommended.
How Do You Write the Subjective Section for Petunia Park?
The Subjective section for Petunia Park documents eight required data categories — and the most common error is omitting any one of them, which drops your score by a full tier on the rubric.
Chief Complaint
Record in the patient’s own words, in quotation marks: “My medicine squashes who I am — and then I crash so low I can’t get out of bed for weeks.”
This direct quote serves two clinical purposes: it documents the presenting concern accurately, and it signals ambivalence about medication adherence — a target for motivational interviewing in the Plan section.
History of Present Illness (HPI)
The HPI must address: onset, duration, severity, quality, location (not applicable here), associated symptoms, modifying factors, and functional impact. For mood disorders, the chronological mood history is the critical component.
Document the alternating pattern explicitly: elevated phases (decreased sleep to 2–4 hours with perceived energy, increased goal-directed activity, impulsivity including spending) lasting approximately 1–2 weeks; depressive phases (hypersomnia 12–16 hours, hyperphagia, anhedonia, fatigue, poor concentration) lasting approximately 4–8 weeks. Onset: adolescence. Current phase: transitioning from elevated to depressive.
Medication History: What to Document When Specifics Are Unavailable
The video does not name the patient’s current medication. This is intentional — it tests whether you recognize the gap and address it clinically rather than fabricating details.
Document: “Current mood stabilizer and/or antipsychotic — specific agent, dose, frequency, and duration not confirmed during session. Medication reconciliation required at next contact.” Note the patient’s subjective experience of the medication as relevant to adherence.
Laboratory Data: What Each Value Means
- Urine drug and alcohol screen: Negative — rules out substance-induced mood disorder as primary diagnosis
- CBC, CMP, lipid panel: Within normal limits — rules out anemia, metabolic disorder, and hyperlipidemia as contributors to fatigue and mood symptoms
- Prolactin: 8 ng/mL (normal) — rules out hyperprolactinemia from antipsychotic use, which can present with mood symptoms
- TSH: 6.3 mIU/L (HIGH) — subclinical hypothyroidism; clinically significant; must be addressed in Assessment and Plan
What Should the Plan Include to Score Full Marks?
A full-marks Plan section names specific interventions with evidence-based rationale — generic statements like ‘prescribe a mood stabilizer’ earn partial credit at best and demonstrate inadequate clinical specificity.
Psychotherapy: Which Modality and Why
Cognitive Behavioral Therapy (CBT) adapted for bipolar disorder is the highest-evidence psychotherapeutic intervention for this population. A 2003 randomized controlled trial by Lam et al. demonstrated that CBT significantly reduced relapse rates and hospitalization frequency in Bipolar I patients over an 18-month follow-up period compared to treatment-as-usual alone.
Interpersonal and Social Rhythm Therapy (IPSRT) is a strong alternative — developed specifically for bipolar disorder, it stabilizes daily routines (sleep-wake cycles, meal timing, activity levels) that are dysregulated in this patient population. Frank et al. (2005) demonstrated superior 2-year outcomes for patients receiving IPSRT plus pharmacotherapy versus pharmacotherapy alone.
Pharmacology: What to Prescribe and Why
Do not prescribe antidepressant monotherapy for a patient with Bipolar I Disorder. Antidepressants without concurrent mood stabilization increase the risk of a manic switch — the American Psychiatric Association’s Practice Guideline for Bipolar Disorder explicitly cautions against this (American Psychiatric Association, 2022).
First-line pharmacotherapy options for bipolar depression include quetiapine (Seroquel) (FDA-approved for bipolar I depression, Level 1 evidence), lurasidone (Latuda) (FDA-approved for bipolar I depression in adults), and lithium carbonate with or without lamotrigine augmentation. A specific prescribing example:
| Sample Pharmacologic Plan: Quetiapine XR 50 mg PO QHS; titrate by 50 mg every 3–4 days as tolerated; target dose 150–300 mg nightly for bipolar depression. Rationale: FDA-approved indication, Level 1 evidence (Calabrese et al., 2005), lower manic switch risk versus antidepressants. Monitoring: metabolic panel (weight, fasting glucose, HbA1c, lipids) at baseline and every 3 months. Assess for EPS, orthostatic hypotension, sedation at each follow-up. |
Patient Education Strategy: Name It Specifically
The rubric requires one named patient education strategy — not a general statement about ‘educating the patient.’ The teach-back method is the highest-evidence patient education intervention for medication adherence and health literacy (Agency for Healthcare Research and Quality, 2020).
Document it as: “Psychoeducation delivered using the teach-back method: patient asked to explain in her own words the importance of sleep schedule regularity as a mania trigger, and to identify three warning signs of an emerging manic episode. Response documented.”
Health Promotion: Address the Blood Pressure
Blood pressure of 138/88 mmHg meets AHA/ACC criteria for Stage 1 hypertension (Whelton et al., 2018) — a finding present in the objective data that must be addressed in the Plan. Document a referral to primary care for hypertension monitoring, DASH diet counseling, and sodium restriction. Cardiovascular disease is a leading cause of premature mortality in patients with bipolar disorder, with standardized mortality ratios 1.5–2 times that of the general population (Crump et al., 2013).
How Do You Write the Reflection Section at the Advanced Level?
The Reflection section is where the majority of students underperform — the rubric explicitly states it must go ‘beyond confidentiality and consent,’ yet most submissions address nothing else.
Legal and Ethical Considerations Beyond Consent
Three ethical issues are directly relevant to this case and go beyond boilerplate confidentiality discussion:
- Autonomy versus beneficence in medication decisions — Petunia Park’s explicit statement that medication ‘squashes who she is’ represents a documented conflict between her autonomy (the right to refuse medication) and the clinician’s duty of beneficence (preventing the documented harms of untreated Bipolar I, including neurotoxic effects of repeated manic episodes on hippocampal volume per Berk et al., 2011). A shared decision-making model is the ethically appropriate resolution — not paternalistic insistence or passive accommodation of non-adherence.
- Duty to protect — proactive safety planning — while no current suicidal ideation is present, a patient with a history of inpatient psychiatric admissions and a current depressive episode requires a formal safety plan documented in the chart. Failure to complete this constitutes a clinical and legal gap, regardless of the patient’s current denial of intent.
- Financial impulsivity during manic phases as a vulnerability factor — the patient reports spending sprees during elevated phases. This creates potential financial exploitation risk and access barriers to care. A social work referral for case management, pharmaceutical assistance programs, and financial counseling addresses both ethical obligations (beneficence, justice) and practical clinical management.
Cultural and Socioeconomic Factors to Address
As a 29-year-old Caucasian female, this patient sits within a demographic that is statistically more likely to be diagnosed with MDD and less likely to be diagnosed with Bipolar I — even when presenting with documented cyclical mood disorder (Bauer et al., 2008). Clinician bias toward depression diagnoses in young Caucasian women is a documented phenomenon that the PMHNP must actively counteract through adherence to DSM-5 criteria rather than clinical impression.
Socioeconomic instability — inconsistent employment and impulsive financial decisions — creates concrete barriers to medication adherence (cost), consistent outpatient follow-up (transportation, time), and therapeutic engagement. The Plan must address these barriers explicitly, not assume them away.
What Are the Rubric Requirements That Most Students Miss?
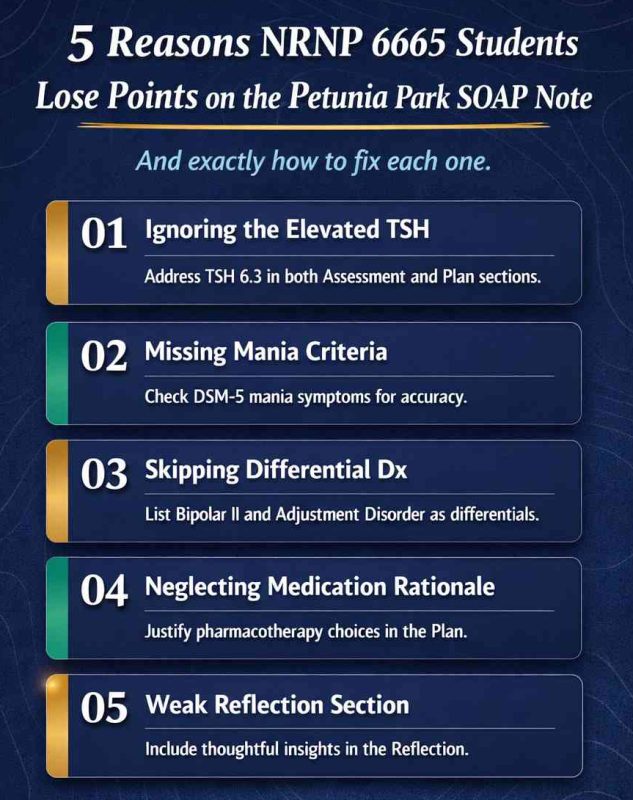
Six specific rubric requirements account for the majority of avoidable point losses on this assignment — and every one of them can be addressed with targeted additions to your submission.
1. DSM-5 Ruling-Out Logic for Each Differential
Naming three disorders is not sufficient. The rubric requires that you cite the DSM-5 criterion that excludes each non-primary differential. For MDD, that criterion is DSM-5 Criterion D (296.32): ‘The episode is not attributable to the physiological effects of a substance or another medical condition, and is not better explained by… a manic or hypomanic episode.’
2. The Elevated TSH Must Be Clinically Addressed
Simply listing ‘TSH 6.3 (H)’ in the Objective section is not sufficient. The Assessment must explain its clinical significance — contribution to depressive symptoms, relevance to mood stabilizer prescribing — and the Plan must include thyroid follow-up orders (Free T4, anti-TPO antibodies, PCP referral).
3. Pharmacology Must Name Agents, Doses, and Monitoring
‘Prescribe a mood stabilizer’ loses points. ‘Quetiapine XR 50 mg PO QHS, titrate to 150–300 mg nightly for bipolar depression, with baseline and quarterly metabolic monitoring’ earns full marks. The rubric scores pharmacologic rationale, not just pharmacologic intent.
4. The Reflection Must Include Three Distinct Elements
- Legal/ethical considerations beyond confidentiality and consent — the rubric states this explicitly
- Health promotion with patient-specific factors (age, ethnicity, PMH, socioeconomic status)
- Disease prevention addressing risk factors, not just generic wellness recommendations
5. A Specific Named Patient Education Strategy
‘Patient education regarding her diagnosis’ fails the rubric. ‘Psychoeducation using the teach-back method, documented with patient’s verbatim response to the teach-back question’ meets the rubric’s requirement for specificity.
6. APA 7th Edition Formatting — Specific Errors to Avoid
- Running head: removed in APA 7th edition — do not include it
- DOI required for all journal articles — ‘Retrieved from’ is not acceptable in APA 7
- References formatted with hanging indent and double spacing
- No page numbers on in-text citations for paraphrased content (only for direct quotes)
How to Write This Assignment Efficiently — A 5-Step Process for Working Nurses
PMHNP students in full-time clinical roles need a replicable, time-efficient process — not a reminder to ‘review the learning resources.’
- Watch the video with the rubric open. Take notes directly under each SOAP heading as you watch. Do not watch once for content and once for notes — structure your first viewing around the deliverable.
- Write the Objective section first. It is the most concrete. Transcribe all vital signs and laboratory values. Interpret the TSH. Document your MSE observations systematically using the standard MSE categories (appearance, behavior, speech, mood, affect, thought process, thought content, perceptual disturbances, cognition, insight, judgment).
- Build the Assessment using the DSM-5 directly. Look up criteria for Bipolar I, Bipolar II, and MDD. Write the ruling-out language for each differential in your own words but cite the specific DSM-5 section. This is the most time-consuming section — budget 40% of your writing time here.
- Write the Plan last, before the Reflection. Use the structure: psychotherapy → pharmacology (named agent, dose, monitoring) → nonpharmacologic interventions → follow-up parameters → health promotion activity → patient education strategy. Check each item against the rubric before moving on.
- Write the Reflection with a checklist. Before submitting, verify: Does my reflection address (a) at least one ethical issue beyond consent? (b) At least one cultural or socioeconomic factor specific to this patient? (c) A disease prevention recommendation with a stated patient-specific rationale? If not, add it before submitting.
References
American Psychiatric Association. (2022). Diagnostic and statistical manual of mental disorders (5th ed., text revision). American Psychiatric Publishing. https://doi.org/10.1176/appi.books.9780890425787
Bauer, M., Goetz, T., Glenn, T., & Whybrow, P. C. (2008). The thyroid-brain interaction in thyroid disorders and mood disorders. Journal of Neuroendocrinology, 20(10), 1101–1114. https://doi.org/10.1111/j.1365-2826.2008.01774.x
Berk, M., Kapczinski, F., Andreazza, A. C., Dean, O. M., Giorlando, F., Maes, M., Yücel, M., Gama, C. S., Dodd, S., Dean, B., Magalhães, P. V. S., Amminger, P., McGorry, P., & Malhi, G. S. (2011). Pathways underlying neuroprogression in bipolar disorder: Focus on inflammation, oxidative stress and neurotrophic factors. Neuroscience and Biobehavioral Reviews, 35(3), 804–817. https://doi.org/10.1016/j.neubiorev.2010.10.001
Calabrese, J. R., Keck, P. E., Jr., Macfadden, W., Minkwitz, M., Ketter, T. A., Weisler, R. H., Cutler, A. J., McCoy, R., Wilson, E., & Mullen, J. (2005). A randomized, double-blind, placebo-controlled trial of quetiapine in the treatment of bipolar I or II depression. American Journal of Psychiatry, 162(7), 1351–1360. https://doi.org/10.1176/appi.ajp.162.7.1351
Crump, C., Sundquist, K., Winkleby, M. A., & Sundquist, J. (2013). Comorbidities and mortality in bipolar disorder: A Swedish national cohort study. JAMA Psychiatry, 70(9), 931–939. https://doi.org/10.1001/jamapsychiatry.2013.1394
Frank, E., Kupfer, D. J., Thase, M. E., Mallinger, A. G., Swartz, H. A., Fagiolini, A. M., Grochocinski, V., Houck, P., Scott, J., Thompson, W., & Monk, T. (2005). Two-year outcomes for interpersonal and social rhythm therapy in individuals with bipolar I disorder. Archives of General Psychiatry, 62(9), 996–1004. https://doi.org/10.1001/archpsyc.62.9.996
Garber, J. R., Cobin, R. H., Gharib, H., Hennessey, J. V., Klein, I., Mechanick, J. I., Pessah-Pollack, R., Singer, P. A., & Woeber, K. A. (2012). Clinical practice guidelines for hypothyroidism in adults. Thyroid, 22(12), 1200–1235. https://doi.org/10.1089/thy.2012.0205
Lam, D. H., Watkins, E. R., Hayward, P., Bright, J., Wright, K., Kerr, N., Parr-Davis, G., & Sham, P. (2003). A randomized controlled study of cognitive therapy for relapse prevention for bipolar affective disorder. Archives of General Psychiatry, 60(2), 145–152. https://doi.org/10.1001/archpsyc.60.2.145
Livingstone, C., & Rampes, H. (2006). Lithium: A review of its metabolic adverse effects. Journal of Psychopharmacology, 20(3), 347–355. https://doi.org/10.1177/0269881105057opposit6192
Whelton, P. K., Carey, R. M., Aronow, W. S., Casey, D. E., Jr., Collins, K. J., Dennison Himmelfarb, C., DePalma, S. M., Gidding, S., Jamerson, K. A., Jones, D. W., MacLaughlin, E. J., Muntner, P., Ovbiagele, B., Smith, S. C., Jr., Spencer, C. C., Stafford, R. S., Taler, S. J., Thomas, R. J., Williams, K. A., Sr., … Wright, J. T., Jr. (2018). 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults. Journal of the American College of Cardiology, 71(19), e127–e248. https://doi.org/10.1016/j.jacc.2017.11.006
Frequently Asked Questions
What is the correct primary diagnosis for Petunia Park in NRNP 6665?
The correct primary diagnosis is Bipolar I Disorder, Most Recent Episode Depressed (DSM-5 296.52 / F31.32) with the specifier ‘with anxious distress.’ The diagnosis is supported by the patient’s documented history of full manic episodes requiring inpatient hospitalization and a current major depressive episode meeting DSM-5 criteria. Bipolar II is ruled out because at least one full manic episode has occurred; MDD is ruled out by the presence of lifetime manic episodes.
Why does the elevated TSH of 6.3 matter for this SOAP note?
A TSH of 6.3 mIU/L indicates subclinical hypothyroidism, which can worsen depressive symptoms including fatigue, hypersomnia, and cognitive slowing. It is also clinically important because lithium — a first-line mood stabilizer for Bipolar I — induces hypothyroidism in 20–40% of patients. The TSH must be addressed in both the Assessment (as a pertinent positive) and the Plan (with orders for Free T4, anti-TPO antibodies, and PCP referral).
What are the three required differential diagnoses for this assignment?
The three differentials listed in order from highest to lowest priority are: (1) Bipolar I Disorder as the primary diagnosis; (2) Bipolar II Disorder, ruled out by the documented history of full manic episodes requiring hospitalization; and (3) Major Depressive Disorder, ruled out by DSM-5 Criterion D, which excludes MDD when manic or hypomanic episodes are present. Each differential must include the specific DSM-5 criterion that supports and excludes it.
What does ‘beyond confidentiality and consent’ mean in the reflection section?
The rubric explicitly instructs students to demonstrate ethical critical thinking beyond basic confidentiality and HIPAA compliance. Advanced ethical considerations for this case include the tension between patient autonomy and beneficence regarding medication that the patient experiences as identity-altering, duty-to-protect safety planning obligations, diagnostic bias affecting young Caucasian women with bipolar spectrum disorders, and socioeconomic barriers to medication adherence and follow-up care.
What pharmacologic treatment should be included in the Plan?
The Plan should not include antidepressant monotherapy, which risks precipitating a manic switch in Bipolar I. Evidence-based options include quetiapine (Seroquel) 50–300 mg nightly (FDA-approved for bipolar I depression), lurasidone (Latuda) 20–120 mg daily with food (FDA-approved), or lithium carbonate at therapeutic serum levels (0.6–1.2 mEq/L for maintenance). Each agent must be documented with starting dose, target dose, indication, and monitoring parameters.
How long should the NRNP 6665 Week 4 SOAP note be?
Walden University’s rubric does not specify a minimum word count for the SOAP note itself, but high-scoring submissions typically run 2,500–4,000 words inclusive of all sections. The Assessment section is the most heavily weighted and requires the greatest depth; plan for it to be your longest section. The Reflection section should be substantive enough to address ethical, cultural, and health promotion elements; typically 400–600 words.
Author Bio
| The author is a board-certified Psychiatric Mental Health Nurse Practitioner with 6 years of clinical experience in inpatient and outpatient psychiatric settings, specializing in mood disorders and psychopharmacology. This article reflects current DSM-5-TR diagnostic standards, APA 7th edition formatting requirements, and evidence-based pharmacotherapy guidelines as of the publication date. |
Article Update Log
| Date | Update Summary |
| June 5, 2026 | Initial publication: comprehensive article covering NRNP 6665 Week 4 Petunia Park SOAP note, including primary diagnosis (Bipolar I, DSM-5 296.52), DSM-5 differential reasoning, TSH clinical interpretation, full pharmacotherapy plan with evidence-based references, ethical/cultural reflection guidance, and FAQ |
This guide seems pretty detailed. Is there a specific part of the SOAP note that you find most tricky?