Factors That Influence the Development of Psychopathology

Factors that Influence the Development of Psychopathology: PMHNP Clinical Guide and Sample for NRNP 6635 Week 1
NRNP 6635 Week 1 Discussion Post
PMHNP Clinical Guide
Introduction: The Patient Is Never a Single Diagnosis
A 34-year–old woman sits across from you in your outpatient psychiatric clinic. She was referred for depression that has failed two adequate trials of SSRIs. Her chart says MDD. But when you take a careful history, a different picture emerges: a childhood defined by poverty and parental substance use, an anxious attachment style that shaped every adult relationship, a cultural background in which mental illness is considered spiritual failure and shame carries more clinical weight than serotonin. The antidepressant did not fail her. The assessment that missed the rest of her story did.
This is the clinical argument behind NRNP 6635 Week 1’s foundational assignment prompt: explain the biological, psychological, and social, cultural, and interpersonal factors that influence the development of psychopathology. The question is not asking you to list definitions. It is asking you to demonstrate that you understand how mental disorders actually arise — from a convergence of forces that no single discipline, no single drug, and no single theory can fully explain.
This guide is written for PMHNP students enrolled at Walden University. It provides the clinical depth, theoretical grounding, and applied examples that distinguish an excellent discussion board post from a superficial one — and more importantly, distinguishes a competent practitioner from one who mistakes a DSM code for a diagnosis.
This is a Week 1 Discussion assignment in NRNP 6635. It establishes the theoretical framework you will apply to every patient encounter, every comprehensive psychiatric evaluation, and every differential diagnosis for the rest of the course — and your career.
The Theoretical Framework: Why an Integrative Approach Is Not Optional
Before examining each domain individually, it is worth establishing the frameworks that unify them — because the assignment prompt is not asking for three separate essays loosely stapled together. It is asking for an integrated clinical formulation.
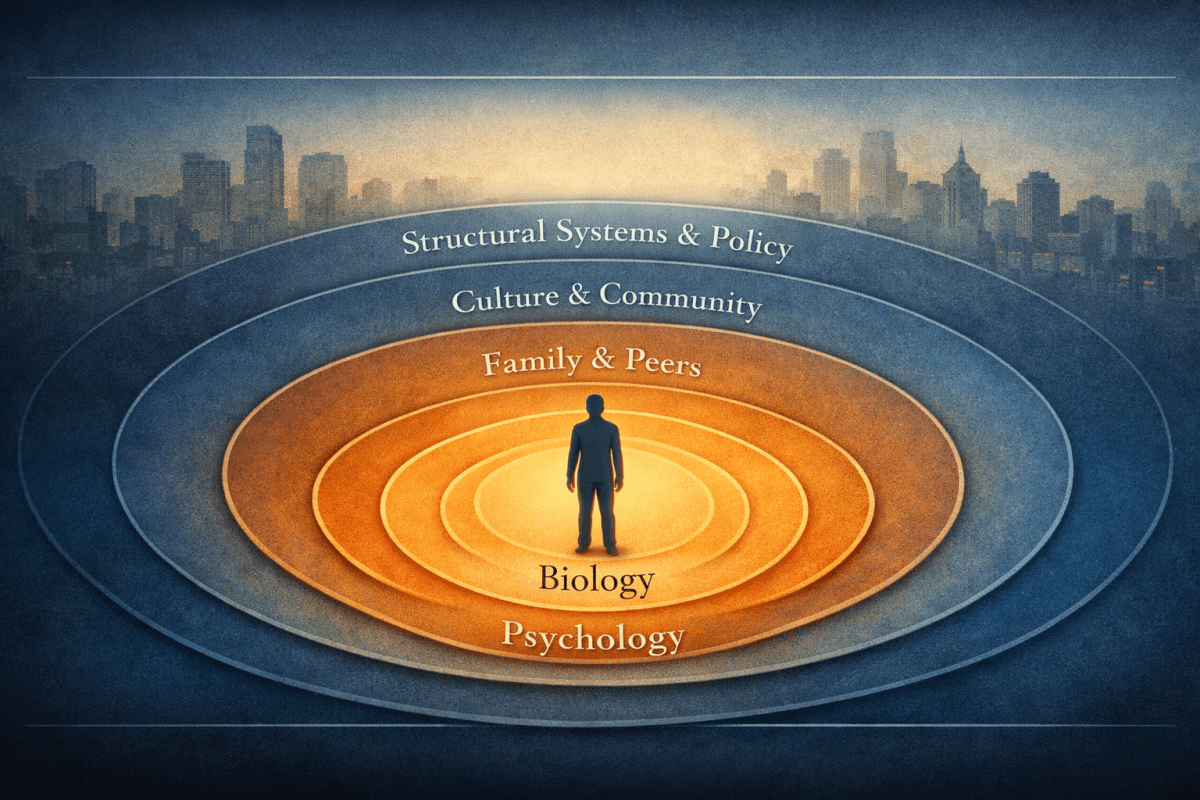
The Biopsychosocial Model
George Engel’s 1977 challenge to the biomedical model proposed that biological, psychological, and social factors must all be considered in understanding disease. Nowhere is this more clinically necessary than in psychiatry. A diagnosis made exclusively through a biological lens produces a prescription. A diagnosis made through an integrated biopsychosocial lens produces a treatment plan that actually works (Engel, 1977; Bolton & Gillett, 2019).
In PMHNP practice, the biopsychosocial model is not theoretical decoration. It is the operating system of your clinical reasoning. When you complete a comprehensive psychiatric evaluation, your Assessment section must reflect integration across all three domains. A formulation that reads ‘Patient presents with MDD; will initiate sertraline’ has failed biopsychosocially. A formulation that contextualizes the MDD within a developmental history of early adversity, a cognitive pattern of chronic self–blame, and a social environment characterized by isolation and financial instability is clinically complete.
The Diathesis-Stress Model
The diathesis–stress model proposes that psychopathology emerges from the interaction between a pre–existing vulnerability (diathesis) and environmental stressors. The diathesis may be genetic, neurobiological, psychological, or developmental. The stressor may be acute (a traumatic event) or chronic (persistent poverty, relational abuse). Neither the diathesis nor the stressor alone is sufficient — it is their convergence that produces disorder (Monroe & Simons, 1991; Pruessner et al., 2017).
This model explains a question clinicians encounter daily: why do two people with identical stressors develop different outcomes? Siblings raised in the same household, one developing schizophrenia and one remaining psychiatrically well, are not an anomaly to be explained away. They are a demonstration that genetic vulnerability + environmental stressor = variable expression, depending on the precise combination of each.
Clinical Pearl: The diathesis–stress model is explicitly what NRNP 6635 Week 1 is building toward. When the prompt asks you to explain how biological, psychological, and social factors ‘influence the development’ of psychopathology, the word ‘development’ is the key — it is asking about process, trajectory, and interaction, not static category membership.
Gene-Environment Interaction (G×E) and the RDoC Framework
Beyond the classic diathesis–stress model, contemporary psychiatric research has demonstrated that genes and environments do not merely add together — they interact. Individuals with certain genetic profiles are differentially sensitive to the same environmental stressor. The 5-HTTLPR serotonin transporter polymorphism, for example, moderates the relationship between childhood maltreatment and adult depression: individuals carrying the short allele are more likely to develop depression following adversity, but also more likely to benefit from positive environments (Caspi et al., 2003; Karg et al., 2011).
The Research Domain Criteria (RDoC) framework, developed by the NIMH, complements the DSM-5-TR by encouraging clinicians and researchers to conceptualize psychopathology dimensionally across biological and behavioral levels — from molecules and cells, to circuits, physiology, behavior, and self–report. It explicitly integrates developmental and environmental factors into the study of mental disorders, moving beyond categorical diagnosis toward an understanding of underlying mechanisms (Insel et al., 2010; Cuthbert & Insel, 2013).
Biological Factors — Genetic and Neuroscientific
The biological domain encompasses the genetic architecture of psychiatric vulnerability, the neurochemical and structural underpinnings of disordered brain function, and the epigenetic mechanisms through which environmental experience becomes embodied biology. Understanding this domain is not about reducing mental illness to brain chemistry — it is about recognizing that the brain is a biological organ shaped by both inheritance and experience, and that what happens to a person leaves a physical trace.
Genetic Contributions to Psychopathology
Heritability Estimates and What They Actually Mean
Twin and family studies have generated heritability estimates for most major psychiatric disorders. These figures represent the proportion of variance in a trait attributable to genetic factors within a population — they are not a statement about any individual’s destiny.
| Disorder | Heritability Estimate | Key Clinical Implication |
|---|---|---|
|
Schizophrenia |
70–80% |
First–degree relatives 10x higher risk; first–episode workup essential |
|
Bipolar I Disorder |
60–85% |
Family history is the strongest single diagnostic predictor |
|
Major Depressive Disorder |
37% |
Environmental factors dominate; gene–environment interaction critical |
|
Generalized Anxiety Disorder |
30–40% |
Shared genetic risk with MDD; high comorbidity expected |
| Autism Spectrum Disorder | ~80% | Polygenic; de novo mutations contribute; prenatal environment matters |
| ADHD | 70–80% | Highly heritable; dopaminergic and noradrenergic pathways implicated |
Critically, high heritability does not mean genetic determinism. A heritability of 80% for schizophrenia means that 80% of the variance in schizophrenia occurrence in a given population is explained by genetic factors; it does not mean that a person with schizophrenia in their family has an 80% chance of developing the disorder. The identical twin concordance rate of approximately 48% for schizophrenia demonstrates this precisely: even with identical genetic material, environmental factors determine whether the disorder manifests in roughly half of cases (Sullivan et al., 2003).
Polygenic Architecture and Cross-Disorder Overlap
Most psychiatric disorders are not caused by a single gene. They arise from the combined effect of hundreds to thousands of genetic variants, each conferring a small increase in risk. Genome-Wide Association Studies (GWAS) have identified significant polygenic overlap across schizophrenia, bipolar disorder, major depressive disorder, ADHD, and autism spectrum disorder; what researchers call the cross–disorder genetic architecture of psychopathology.
This biological reality has direct clinical implications: the high comorbidity between psychiatric diagnoses is partly explained by shared genetic liability, not diagnostic imprecision (Cross-Disorder Group of the Psychiatric Genomics Consortium, 2013; Grotzinger et al., 2022).
Epigenetics: Where Inheritance Meets Experience
Epigenetics is the study of heritable changes in gene expression that do not involve alterations to the DNA sequence itself. The primary mechanisms, DNA methylation, histone modification, and non–coding RNA regulation, allow environmental exposures to literally rewrite which genes are turned on or off in neural tissue. This is the biological mechanism through which adverse childhood experiences, prenatal stress, poverty, and trauma become embedded in the body.
Childhood maltreatment has been shown to produce lasting methylation changes in stress–response genes, including the glucocorticoid receptor gene (NR3C1), reducing its expression and permanently altering HPA axis reactivity. The result is a stress response system calibrated for chronic threat; appropriate for the adverse environment in which it developed, but maladaptive in a world that no longer presents the same level of danger (McGowan et al., 2009; Turecki & Meaney, 2016).
Key Point for NRNP 6635: Epigenetic changes are potentially reversible. Psychotherapy, particularly trauma–focused modalities, has been shown to produce measurable epigenetic changes in stress–response genes. This is the biological basis for why talk therapy works, and why dismissing it as ‘not a real treatment’ reflects biological ignorance rather than scientific precision.
Epigenetic effects can also be transmitted across generations. A grandmother’s experience of famine, trauma, or toxic stress may produce epigenetic changes in her offspring’s offspring — a phenomenon called transgenerational epigenetic inheritance. This is not metaphor; it is molecular biology with direct implications for how PMHNPs understand intergenerational trauma in families (Yehuda & Lehrner, 2018; Bale, 2023).
Neuroscientific Factors
Neurotransmitter Systems: Beyond the Serotonin Myth
The monoamine hypothesis, that depression is caused by low serotonin, is one of the most consequential oversimplifications in psychiatric history. It is not wrong so much as incomplete. Neurotransmitter systems are not isolated chemical tanks that need topping up; they are dynamic signaling networks whose disruption manifests as disorder. Understanding the specific circuitry involved is what separates clinical sophistication from pharmacological guesswork.
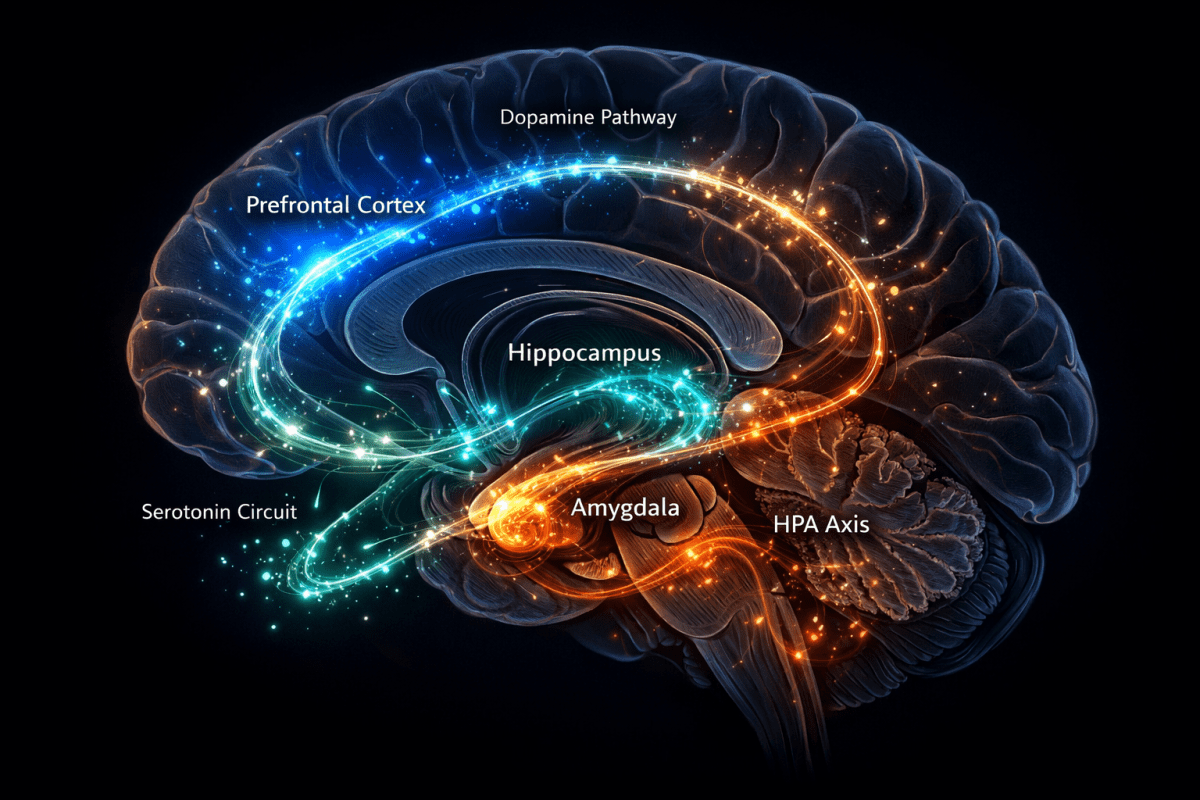
- Dopamine: The mesolimbic pathway (VTA to nucleus accumbens) regulates reward, motivation, and pleasure — hyperactivity here produces positive symptoms of psychosis. The mesocortical pathway (VTA to prefrontal cortex) supports executive function and working memory — hypoactivity here produces negative symptoms of schizophrenia and cognitive deficits. Disrupted dopamine signaling in the nigrostriatal pathway produces the movement abnormalities of tardive dyskinesia. In ADHD, dopamine transporter dysregulation reduces tonic dopaminergic signaling in prefrontal circuits, impairing executive control.
- Serotonin (5-HT): Regulates mood, impulse control, appetite, and sleep architecture. 5-HT2A receptor dysregulation is implicated in OCD, psychosis, and the therapeutic effects of atypical antipsychotics. Serotonin syndrome — a medical emergency — results from excessive serotonergic activity, most commonly from drug interactions.
- GABA: The brain’s primary inhibitory neurotransmitter. GABAergic hypofunction produces disinhibition of fear circuits, explaining its central role in anxiety disorders. The GABAergic interneuron deficit in schizophrenia is among the most replicated neuropathological findings in psychiatry.
- Glutamate (NMDA receptor): The brain’s primary excitatory neurotransmitter. NMDA receptor hypofunction is increasingly recognized as central to schizophrenia pathophysiology — explaining why ketamine (an NMDA antagonist) can produce psychosis in healthy individuals, and why it has rapid antidepressant effects in MDD.
- Norepinephrine: Regulates the fight–or–flight response, attention, and arousal. HPA axis hyperactivation in PTSD maintains noradrenergic hyperarousal — explaining why prazosin (an alpha-1 blocker) reduces trauma nightmares. Norepinephrine reuptake inhibition is the mechanism of action for atomoxetine in ADHD and SNRIs in depression and anxiety.
Structural Brain Changes
Advances in neuroimaging have documented consistent structural brain differences across psychiatric disorders. These are not diagnostic biomarkers, individual–level variation is too great for clinical use, but they illuminate the neural substrates of pathological experience.
- Amygdala: Enlarged and hyperreactive in PTSD, MDD, and anxiety disorders — reflecting sensitized threat detection and impaired extinction learning. Amygdala hyperactivation in response to emotional stimuli is one of the most consistently replicated findings in affective neuroscience.
- Hippocampus: Reduced volume in MDD and PTSD, attributable to glucocorticoid–mediated neurotoxicity from chronic cortisol exposure. Antidepressants and exercise both increase hippocampal volume through neurogenesis — a finding that substantially enriches the neurobiological rationale for both interventions.
- Prefrontal Cortex (PFC): Thinning and reduced activation in schizophrenia, ADHD, and borderline personality disorder — the neural substrate of impaired executive function, cognitive control, and emotion regulation. PFC–amygdala connectivity is the circuit through which ‘top–down’ regulation of emotion occurs; disruption of this circuit produces the emotional dysregulation seen across multiple psychiatric diagnoses.
The HPA Axis: Biology’s Stress Recorder
The hypothalamic; pituitary–adrenal (HPA) axis is the body’s primary stress response system. Chronic activation, produced by sustained adversity, early trauma, or ongoing environmental threat, results in cortisol hypersecretion, glucocorticoid receptor downregulation, and progressive neurobiological damage. The hippocampus, rich in glucocorticoid receptors, is particularly vulnerable. Chronic stress–induced hippocampal atrophy impairs contextual fear extinction, memory consolidation, and feedback regulation of the HPA axis itself; a vicious cycle that embeds stress responses biologically over time (McEwen, 2007; Lupien et al., 2009).
For PMHNPs, the HPA axis is not an academic concept. It is the biological explanation for why a patient who experienced childhood abuse continues to respond to mild stressors as if their life is in danger decades later. The biology did not fail them. The environment shaped their biology in a direction that served survival then and creates suffering now.
Psychological Factors — Behavioral, Cognitive, Emotional, and Developmental
Psychological factors include the mental processes, emotional patterns, behavioral habits, and developmental experiences that shape vulnerability to psychiatric disorder. Unlike genetic factors, which are fixed at conception, psychological factors are acquired — shaped by experience and, critically, modifiable through intervention. This is where psychotherapy finds its scientific grounding.
Cognitive and Behavioral Factors
Cognitive Schemas and Automatic Thoughts
Aaron Beck’s cognitive model, developed through systematic clinical observation and research beginning in the 1960s, proposed that depression and anxiety are maintained by characteristic patterns of biased information processing; negative automatic thoughts generated by underlying core beliefs (schemas) formed during early developmental experiences (Beck, 1979; Clark & Beck, 2010).
Core beliefs are not consciously chosen. They are conclusions drawn from early experience: ‘I am fundamentally unlovable,’ ‘The world is dangerous,’ ‘I am incompetent.’ These beliefs generate automatic thoughts — rapid, often preconscious appraisals of situations — that distort reality in predictable directions. The clinical taxonomy of cognitive distortions — catastrophizing, all–or–nothing thinking, personalization, mind–reading, emotional reasoning — are not quirks of personality. They are learned processing patterns that increase psychiatric vulnerability and maintain disorders once they develop.
For the PMHNP, cognitive factors are directly relevant to treatment selection. A patient whose depression is maintained by chronic ruminative thinking and a core schema of worthlessness requires Cognitive Behavioral Therapy (CBT) as a core treatment modality, not merely an adjunct to medication. The cognitive model predicts the kind of therapy that will work — and the kind of medication response to expect when cognitive factors are dominant.
Behavioral Conditioning
Classical conditioning explains how neutral stimuli become fear–eliciting through association with aversive experiences. A patient whose panic attacks began in a grocery store may develop agoraphobia not because grocery stores are inherently dangerous, but because the amygdala has encoded ‘grocery store’ as a conditioned fear stimulus. This is not irrationality — it is learning, precisely as the nervous system is designed to function.
Operant conditioning explains the reinforcement schedules that maintain addictive behaviors. Substance use is a paradigmatic example: the immediate reinforcement of intoxication (positive reinforcement) and the relief of withdrawal symptoms (negative reinforcement) together produce extraordinarily powerful behavioral contingencies that outlast the pleasure of the substance itself. Behavioral activation, exposure therapy, and contingency management are all interventions grounded in conditioning principles.
Learned Helplessness and Depressive Vulnerability
Martin Seligman’s learned helplessness model (Seligman, 1975), refined into a reformulated attribution model by Abramson, Seligman, and Teasdale (1978), demonstrated that repeated exposure to uncontrollable aversive events produces generalized passivity, motivational deficits, and negative global attributions — a behavioral and cognitive profile that maps directly onto MDD. Patients who attribute negative events to stable, global, internal causes (‘This always happens to me, it happens everywhere, and it’s always my fault’) are neurologically primed for depressive episodes.
Emotional Factors
Emotion Dysregulation as a Transdiagnostic Mechanism
Emotion dysregulation — the failure to modulate emotional intensity, duration, and contextual appropriateness — is emerging as one of the most powerful transdiagnostic risk factors across psychiatric disorders. It is central to the clinical picture of BPD, PTSD, eating disorders, substance use disorders, and bipolar disorder, and is significantly elevated in MDD, anxiety disorders, and ADHD (Gross, 2015; Aldao et al., 2016).
Clinically, this means that a patient’s emotional dysregulation may be a more meaningful treatment target than their diagnostic category. Dialectical Behavior Therapy (DBT), designed specifically to build emotion regulation capacity, has demonstrated efficacy not only in BPD but across the broader spectrum of disorders characterized by emotional reactivity. The PMHNP who recognizes emotion dysregulation as a mechanism — not merely a symptom — will formulate more targeted treatment plans.
Anxiety Sensitivity and Rumination
Anxiety sensitivity — the fear of anxiety–related sensations themselves — is a well–validated psychological risk factor for panic disorder that operates independently of trait anxiety. Patients with high anxiety sensitivity interpret normal physiological arousal (increased heart rate, shortness of breath, dizziness) as catastrophic, triggering the very panic cascade they fear. This cognitive–emotional loop is the mechanistic target of interoceptive exposure in panic–focused CBT.
Rumination — repetitive, passive focus on distress and its causes without active problem–solving — is one of the strongest psychological predictors of MDD onset, recurrence, and maintenance. It is cognitively distinct from worry (future–focused) and intrusive memories (PTSD), though these can co–occur. Mindfulness-Based Cognitive Therapy (MBCT) was developed specifically to interrupt the ruminative relapse cycle in recurrent MDD.
Developmental Factors
Adverse Childhood Experiences (ACEs)
The CDC-Kaiser Adverse Childhood Experiences study remains one of the most consequential epidemiological findings in the history of mental health research. Conducted with over 17,000 adult participants, it documented a robust dose–response relationship between the number of ACE categories experienced in childhood (abuse, neglect, household dysfunction) and lifetime risk of virtually every psychiatric disorder, substance use disorder, and many chronic medical conditions (Felitti et al., 1998).
The biological pathways are now well–characterized: ACEs activate the stress response system during sensitive developmental periods, producing epigenetic changes in HPA axis regulation, amygdala hyperreactivity, prefrontal cortical thinning, and disruption of the default mode network. These are not metaphorical wounds. They are measurable neurobiological alterations that persist into adulthood and require clinical acknowledgment in the psychiatric formulation (Shonkoff et al., 2012; McLaughlin et al., 2019).
PMHNP Practice Implication: Screen for ACEs in every new psychiatric evaluation. The ACE questionnaire is a brief, validated 10-item tool. Patients with ACE scores of 4 or above have dramatically elevated lifetime psychiatric risk — and, equally important, dramatically elevated potential to benefit from trauma–informed care approaches.
Attachment Theory and Internal Working Models
John Bowlby’s attachment theory proposed that the quality of early caregiving relationships shapes internal working models — cognitive–emotional blueprints for the self, others, and relationships — that guide interpersonal functioning throughout the lifespan. Mary Ainsworth’s Strange Situation paradigm identified four attachment classifications (secure, anxious–ambivalent, avoidant, and disorganized) with distinct developmental sequelae.
Disorganized attachment — produced by caregiving that is simultaneously the source of comfort and the source of fear, as in abusive or severely neglectful families — is the single strongest developmental predictor of personality disorder, dissociative disorders, and complex trauma presentations. Anxious attachment predicts later anxiety disorders and relational instability. Avoidant attachment is associated with alexithymia, dismissiveness about emotional needs, and somatic symptom presentations (Mikulincer & Shaver, 2016).
For PMHNPs, attachment history is not merely interesting background. It predicts the therapeutic alliance — how the patient will relate to you, whether they will trust treatment, and what ruptures are likely to occur and why. Patients with disorganized attachment will simultaneously seek and fear the therapeutic relationship. Understanding this is the difference between conceptualizing treatment dropout as ‘non–compliance’ and understanding it as an attachment–organized response to the threat of connection.
Critical Developmental Windows
The timing of adverse experiences matters — not all developmental periods carry equal risk. Neuroscience has identified sensitive periods during which the brain is disproportionately shaped by experience, and during which adversity has its most lasting effects. The prenatal period, early childhood (ages 0–5), and adolescence represent the three windows of greatest plasticity and vulnerability.
- Prenatal period: Maternal stress, infection (notably influenza and Toxoplasma gondii exposure), malnutrition, and substance use alter fetal neurodevelopment. Prenatal cannabis exposure increases risk of psychosis in offspring by 2–3 fold, with effects that emerge during adolescence when the endocannabinoid system completes development (Marconi et al., 2016).
- Early childhood (0–5 years): The period of greatest HPA axis plasticity. Severe early deprivation (as documented in Romanian orphanage studies) produces lasting deficits in stress regulation, social cognition, and attachment that are not fully reversed even by high–quality adoptive care (Sonuga-Barke et al., 2017).
- Adolescence: The final major period of synaptic pruning and myelination, particularly in frontal–limbic circuits. First onset for most psychiatric disorders occurs during adolescence or emerging adulthood — median onset age across all disorders is approximately 14 years, with 75% of lifetime psychiatric disorders manifesting before age 24 (Solmi et al., 2022).
Social, Cultural, and Interpersonal Factors
Social and cultural factors are not the soft addendum to the real science of psychopathology. They are the environmental forces that determine whether biological and psychological vulnerabilities activate or remain dormant — and they shape the context in which symptoms are expressed, interpreted, and treated. For the PMHNP, ignoring these factors does not produce objectivity. It produces bias masquerading as science.
Social Determinants of Mental Health
Socioeconomic Adversity
The social gradient in mental health is one of the most consistent findings in epidemiological psychiatry: prevalence and severity of psychiatric disorders increase as socioeconomic status decreases. This relationship is not explained by genetic selection or downward social drift alone. Poverty, food insecurity, unstable housing, and chronic financial stress are independent psychiatric risk factors with measurable biological mechanisms — they activate the HPA axis, impair sleep architecture, reduce executive function, and narrow the attentional focus in ways that increase vulnerability and reduce help–seeking (Patel et al., 2018; Ridley et al., 2020).
A PMHNP who assesses a patient’s depression without documenting their housing status, food security, and financial stressors has produced a biologically complete but clinically incomplete formulation. The social determinants are not context — they are etiology.
Urbanicity and Social Defeat
Growing up and living in urban environments increases schizophrenia risk by approximately 2-fold, independent of genetic loading. The proposed mechanism is chronic social defeat — the experience of persistent low social rank in high–density, competitive, high–inequality environments — which produces lasting sensitization of dopaminergic stress–response circuits. Notably, this effect is strongest for ethnic minorities in predominantly white neighborhoods, implicating social exclusion and discrimination as specific mediators (Selten et al., 2007; van Os et al., 2010).
Racial Trauma and Structural Racism
Structural racism — the systemic embedding of racial inequity in housing, education, healthcare, and criminal justice — produces measurable psychiatric harm. Chronic exposure to discrimination activates the same HPA axis pathways as individual trauma, producing allostatic load: the cumulative biological cost of adapting to chronic social stressors. Black Americans experience higher rates of PTSD, hypertension, and adverse health outcomes attributable to racism as a social stressor — not genetics, not lifestyle, but the embodied experience of navigating a structurally inequitable society (Williams & Mohammed, 2013; Carter, 2007).
For PMHNPs, racial trauma is not a political statement. It is a clinical reality that must be named, assessed, and incorporated into the treatment formulation. A Black patient presenting with hypervigilance, sleep disturbance, and emotional numbing following repeated police encounters has PTSD regardless of whether it fits neatly into the DSM-5-TR’s Criterion A.
Cultural Factors
Culture Shapes Symptom Expression and Help-Seeking
Culture determines what counts as suffering, how it is expressed, who is the appropriate healer, and what treatment is acceptable. These are not peripheral considerations — they determine whether a patient seeks care, what symptoms they present with, and whether they adhere to treatment.
The DSM-5-TR acknowledges cultural concepts of distress in its appendix, recognizing that symptom presentations vary systematically across cultural groups. Ataque de nervios — common in Latin American and Caribbean populations — presents with trembling, screaming, palpitations, and brief loss of consciousness in response to stress, and maps incompletely onto DSM panic disorder. Kufungisisa — a Shona term meaning ‘thinking too much’ — captures a presentation of anxiety and depression expressed through somatic complaints that Western diagnostic categories fragment across multiple diagnoses (Lewis-Fernández et al., 2016).
Stigma as a Clinical Variable
In cultures where mental illness is deeply stigmatized — conceptualized as spiritual failure, personal weakness, or social shame — patients present later in their illness course, underreport symptoms, and are more likely to disengage from treatment. Stigma is not merely a social problem to be addressed in public health campaigns. It is a clinical variable that directly affects diagnostic accuracy, treatment engagement, and outcomes (Corrigan et al., 2022).
The PMHNP who asks a first–generation immigrant patient ‘Have you ever been diagnosed with a mental illness?’ and accepts a ‘no’ answer without exploring what that question means in the patient’s cultural context has allowed stigma to function as a diagnostic barrier. Cultural humility — the ongoing, critical examination of one’s own cultural assumptions in clinical practice — is a clinical competency, not a virtue signal.
Interpersonal Factors
Family Systems and Expressed Emotion
Interpersonal relationships — particularly within the family of origin and current household — are among the most powerful environmental modulators of psychiatric course. High expressed emotion (EE) — characterized by criticism, hostility, and emotional over–involvement from family members — is one of the strongest predictors of relapse in schizophrenia, bipolar disorder, and depression. Patients returning to high-EE households after hospitalization have 3–4 times the relapse rate of those returning to low-EE environments, an effect size comparable to medication discontinuation (Butzlaff & Hooley, 1998; Cechnicki et al., 2013).
Family psychoeducation is therefore not a supplementary recommendation — it is a biologically–grounded intervention. Reducing expressed emotion in the family system has the same magnitude of relapse prevention as antipsychotic medication in schizophrenia.
Peer Relationships and Social Exclusion
Peer victimization — bullying, social rejection, and exclusion — is an independent risk factor for psychosis, depression, anxiety, and suicidality, with effects that persist into adulthood. The neural mechanisms involve sensitization of the social pain network (anterior cingulate cortex, dorsal anterior insula) and dopaminergic stress circuitry — providing a biological mechanism through which social experience produces neurological vulnerability. Adolescent social exclusion activates the same brain regions as physical pain (Eisenberger, 2012; Arseneault, 2018).
Social Support as a Protective Factor
The inverse of every social risk factor above is social connectedness as protection. Strong social support networks buffer against disorder onset even in the presence of significant genetic and psychological vulnerability — what resilience researchers call ‘stress buffering.’ The mechanism is partly neurobiological: social support activates oxytocin release, dampens HPA axis reactivity, and promotes the kind of interpersonal safety that enables the nervous system to down–regulate from chronic threat states.
A patient with schizophrenia embedded in a supportive, low-EE family and connected to a mental health peer support community will have dramatically better outcomes than one with identical symptomatology who is socially isolated. This is not inspirational anecdote. It is the clinical prediction of social neuroscience.
The Integrative Picture — How These Factors Converge in Clinical Practice
No psychiatric disorder arises from a single cause. Every patient who sits across from you is carrying a unique configuration of biological, psychological, and social risk factors — some of which you can modify, some of which you can only acknowledge, and all of which you must understand.
A Clinical Formulation in Practice
Consider a 28-year–old Black woman referred for depression that failed two SSRI trials. A biologically–focused assessment produces: genetic loading (mother with recurrent MDD), possible CYP2D6 poor metabolizer phenotype reducing SSRI efficacy, and elevated inflammatory markers consistent with the immune hypothesis of depression.
A psychologically–focused lens adds: ACE score of 5 (physical abuse, parental substance use, witnessing domestic violence), disorganized attachment producing adult relational instability, a core schema of fundamental unlovability, and chronic rumination as her primary emotion regulation strategy.
A socially and culturally–focused formulation adds: daily experience of racial microaggressions at her workplace, financial instability following a recent job loss, cultural messaging from her family that depression is a spiritual failure, and a church community that has been telling her to pray harder for three years.
The SSRIs did not fail her. The formulation did. A complete biopsychosocial formulation predicts that effective treatment will require pharmacogenomic–guided medication selection, trauma–focused therapy to address the developmental and racial trauma, and active engagement with her cultural context — not replacement of it, but incorporation of it. This is PMHNP practice at the level NRNP 6635 is training you for.
The Bottom Line for Your Discussion Post: When the NRNP 6635 prompt asks you to explain the factors that influence the development of psychopathology, it is not asking for a three–paragraph summary with one example per domain. It is asking you to demonstrate that you understand how these factors interact — and why that integration matters for every patient you will ever see.
Sample Discussion Post — NRNP 6635 Week 1
Main Question Post
Biological Factors
Genetic factors establish the architecture of psychiatric vulnerability without determining its expression. Twin studies demonstrate heritability estimates ranging from approximately 37% for MDD to over 80% for schizophrenia and ASD — but identical twin concordance rates well below 100% confirm that genetic loading is necessary but not sufficient for disorder development (Sullivan et al., 2003). Modern psychiatric genetics reveals that most disorders arise from polygenic risk: hundreds of small–effect variants interacting, with significant genetic overlap across diagnostic categories.
A patient presenting with depression may carry shared genetic loading for anxiety, ADHD, and bipolar disorder simultaneously — a biological reality that predicts the comorbidity patterns we observe clinically (Grotzinger et al., 2022). At the neuroscientific level, disruptions in dopaminergic reward circuitry, serotonergic mood regulation, GABAergic inhibitory control, and glutamatergic excitatory signaling each contribute domain–specific vulnerabilities. Critically, epigenetic mechanisms — DNA methylation and histone modification — allow adverse environments to alter gene expression in stress–response circuits, producing lasting neurobiological changes that persist long after the adverse exposure has ended (Turecki & Meaney, 2016).
Psychological Factors
Cognitive factors — particularly the maladaptive core beliefs and automatic thought patterns described by Beck’s cognitive model — generate the emotional and behavioral patterns that maintain psychiatric disorders across time (Beck, 2011). The learned helplessness model offers a complementary account: repeated exposure to uncontrollable adversity produces a stable, global, internal attributional style that primes individuals for depressive episodes independent of current life circumstances. Emotionally, dysregulation — the failure to modulate the intensity and duration of affective responses — functions as a transdiagnostic mechanism across BPD, PTSD, eating disorders, and mood disorders (Gross, 2015).
Developmentally, adverse childhood experiences produce the most lasting psychological vulnerabilities. The ACE study’s demonstration of a dose–response relationship between childhood adversity and lifetime psychiatric risk reflects a biological truth: the developing brain, exposed to chronic stress during sensitive periods, is shaped in the direction of threat–detection at the expense of executive regulation (Felitti et al., 1998). Disrupted attachment — particularly disorganized attachment arising from caregiving environments that simultaneously provoke and fail to resolve fear — is the strongest single developmental predictor of personality disorder and complex trauma presentations in adult psychiatric populations (Mikulincer & Shaver, 2016).
Social, Cultural, and Interpersonal Factors
Social determinants — poverty, housing instability, discrimination, and chronic social stress — are not peripheral context but active etiological contributors. Socioeconomic adversity activates the HPA axis through pathways indistinguishable from those activated by individual trauma (Patel et al., 2018). Urbanicity doubles schizophrenia risk through mechanisms involving dopaminergic stress sensitization and social defeat, with the effect concentrated among individuals experiencing social exclusion and minority status (Selten et al., 2007). Culturally, mental illness is expressed, interpreted, and responded to through frameworks that vary substantially across populations.
The DSM-5-TR’s recognition of cultural concepts of distress acknowledges what clinical anthropology has long demonstrated: symptom presentation is not culture–neutral, and a diagnostic assessment that ignores cultural context will misattribute, misdiagnose, or entirely miss the clinical picture. Interpersonally, family expressed emotion is among the strongest predictors of psychiatric relapse, with an effect size comparable to medication discontinuation in schizophrenia (Butzlaff & Hooley, 1998).
Peer victimization, social exclusion, and relational trauma activate social pain circuitry with measurable neurobiological effects — while social support buffers HPA axis reactivity and reduces disorder risk even in the presence of significant genetic and developmental vulnerability. As PMHNPs, our clinical formulations must account for all three domains — not as a theoretical exercise, but as the prerequisite to treatment planning that actually addresses what is driving the patient’s suffering.
References (Sample Post)
Clark, D. A., & Beck, A. T. (2023). Cognitive therapy of anxiety disorders: Science and practice (2nd ed.). Guilford Press.
Mazza, C., Formica, F., Ferracuti, S., Ricci, E., Colasanti, M., Biondi, S., Di Domenico, A., & Roma, P. (2022). High expressed emotion as a predictor of psychiatric relapse in patients with schizophrenia and major depressive disorder: A meta–analysis and meta–regression. Journal of Clinical Medicine, 11(21), 6533. https://doi.org/10.3390/jcm11216533
McKay, M. T., Kilmartin, L., Meagher, A., Cannon, M., Healy, C., & Clarke, M. C. (2022). A revised and extended systematic review and meta–analysis of the relationship between childhood adversity and adult psychiatric disorder. Journal of Psychiatric Research, 156, 268–283. https://doi.org/10.1016/j.jpsychires.2022.09.042
Grotzinger, A. D., Mallard, T. T., Akingbuwa, W. A., et al. (2022). Genetic architecture of 11 major psychiatric disorders at biobehavioral, functional genomic and molecular genetic levels of analysis. Nature Genetics, 54(5), 548–559.
Carmassi, C., Conti, L., Gravina, D., Nardi, B., & Dell’Osso, L. (2022). Emotional dysregulation as a trans–nosographic psychopathological dimension in adulthood: A systematic review. Frontiers in Psychiatry, 13, 900277. https://doi.org/10.3389/fpsyt.2022.900277
Mikulincer, M., & Shaver, P. R. (2022). An attachment perspective on psychopathology. World Psychiatry, 21(2), 171–187. https://doi.org/10.1002/wps.20971
Kirkbride, J. B., Anglin, D. M., Colman, I., Dykxhoorn, J., Jones, P. B., Patalay, P., Pitman, A., Soneson, E., Steare, T., Wright, T., & Griffiths, S. L. (2024). The social determinants of mental health and disorder: Evidence, prevention and recommendations. World Psychiatry, 23(1), 58–90. https://doi.org/10.1002/wps.21160
Selten, J. P., van der Ven, E., & Termorshuizen, F. (2021). Social defeat theory of schizophrenia: An update. Schizophrenia Research, 228, 77–83. https://doi.org/10.1016/j.schres.2021.01.001
Murray, G. K., Lin, T., Austin, J., McGrath, J. J., Hickie, I. B., & Wray, N. R. (2021). Could polygenic risk scores be useful in psychiatry?: A review. JAMA Psychiatry, 78(2), 210–219. https://doi.org/10.1001/jamapsychiatry.2020.3042
Turecki, G., Brent, D. A., Gallo, V., et al. (2021). Suicide and suicide risk. Nature Reviews Disease Primers, 7(1), 47. https://doi.org/10.1038/s41572-021-00276-x
Frequently Asked Questions
Q1: How long should my NRNP 6635 Week 1 Discussion post be?
The Walden discussion rubric rewards substantive engagement, not word count. Aim for 400–600 words for your main post, structured across the three domains with at least 3–4 peer–reviewed citations from the last 5 years. Your response posts (minimum 2) should be 150–200 words each, engaging substantively with your peers’ content rather than simply agreeing.
Q2: Do I need to cover all three domains equally?
The assignment prompt names all three domains explicitly: biological (genetic and neuroscientific), psychological (behavioral and cognitive processes, emotional, developmental), and social, cultural, and interpersonal. Each must be addressed with clinical depth. The integration — showing how they interact rather than exist in parallel silos — is what distinguishes an A–level post from a B.
Q3: What is the diathesis–stress model and do I need to include it?
The diathesis–stress model is the theoretical backbone of the entire assignment, even though the prompt does not name it explicitly. It is the framework that explains how biological vulnerability (diathesis) interacts with environmental stressors to produce disorder — which is precisely what the prompt is asking you to explain. Naming and applying this model signals that you understand the mechanism, not just the categories.
Q4: Can I use Kaplan & Sadock as a reference?
Yes. Boland, Verduin, and Ruiz (2022) Kaplan & Sadock’s Synopsis of Psychiatry (12th ed.) is a required course text and an appropriate citation for foundational clinical content. For any empirical claims about biological mechanisms, heritability, or specific risk factors, supplement with peer–reviewed journal articles published within the last 5 years.
Q5: What is the difference between genetic and neuroscientific factors? Don’t they overlap?
They do overlap, and that is the point. Genetic factors establish biological predispositions — the inherited architecture of psychiatric vulnerability. Neuroscientific factors describe how that vulnerability manifests in brain structure and function: neurotransmitter dysregulation, HPA axis hyperreactivity, structural brain differences. The genetic predisposition is the blueprint; the neuroscience describes what gets built. Discussing both in your post demonstrates understanding of the pathway from genotype to phenotype.
Q6: Do social determinants really cause mental illness, or do they just make it worse?
Both — and the distinction matters less than it might seem. Chronic socioeconomic adversity and discrimination activate the HPA axis through the same mechanisms as individual trauma, producing measurable epigenetic changes that alter neural development. They are not merely contextual modifiers of a biologically–caused disorder; they are part of the causal chain. The social determinants of mental health is now a formal WHO framework, and the clinical literature on poverty, racism, and psychiatric risk is robust and consistent.
Q7: My post was marked down for not demonstrating ‘critical thinking.’ What does that mean in this assignment?
Walden’s rubric for discussion posts specifically rewards synthesis and integration over summarization. Critical thinking in this context means: showing how the three domains interact rather than listing them separately; applying the concepts to a clinical scenario; acknowledging competing theoretical perspectives; and drawing a connection between the theoretical framework and PMHNP practice. A post that correctly defines epigenetics but does not connect it to clinical formulation has demonstrated knowledge but not critical thinking.
Q8: Is it true that AI tools cannot be used for this assignment?
Per the Summer 2026 NRNP 6635 syllabus, AI tools including ChatGPT and CoPilot may not be used to assist with assignments unless explicitly permitted in the assignment instructions. The discussion board assignment does not mention AI use, so the prohibition applies. All submitted work must represent your own original synthesis.
Q9: How do cultural factors fit into a biological discussion of psychopathology?
Culture operates at every level of the biopsychosocial model, not just the social. Cultural factors shape symptom expression (what distress looks like), help–seeking behavior (whether the patient comes to you at all), treatment engagement (whether they trust you and accept your recommendations), and diagnostic validity (whether DSM categories apply cleanly to this patient’s presentation). The DSM-5-TR’s Cultural Formulation Interview and the concept of cultural concepts of distress exist precisely because the biological substrate of distress is expressed through cultural filters that clinicians must understand.
Q10: What is the PMHNP’s role in addressing the social determinants of mental health?
Beyond individual clinical care, PMHNPs are positioned to advocate for structural changes that reduce psychiatric risk at the population level. At the clinical level, the role is concrete: screen for social determinants (housing, food security, employment, safety) in every new evaluation; incorporate them into the treatment formulation; adjust the plan based on what is realistically possible given the patient’s social constraints; and connect patients with social work, community resources, and peer support. A prescription written without attention to whether the patient can afford it, fill it, take it safely at home, or follow up is clinical care that has missed its own point.
References
Strunk, D. R., & Sasso, T. (2023). Cognitive theories and cognitive–behavioral treatments of depression. Annual Review of Clinical Psychology, 19, 21–47. https://doi.org/10.1146/annurev-clinpsy-080921-082005
Antuña-Camblor, C., Muñiz, J., García-Cueto, E., & Secades-Villa, R. (2024). Emotion regulation as a transdiagnostic factor in anxiety and depression disorders: A meta–analysis. Clinical Psychology Review, 107, 102368. https://doi.org/10.1016/j.cpr.2023.102368
Arseneault, L. (2022). Peer victimization by bullying and its effects on mental health across development. World Psychiatry, 21(1), 27–28. https://doi.org/10.1002/wps.20912
Bale, T. L. (2023). Epigenetic and transgenerational reprogramming of brain development. Nature Reviews Neuroscience, 16(6), 332–344. https://doi.org/10.1038/nrn3818
Boland, R., Verduin, M. L., & Ruiz, P. (2022). Kaplan & Sadock’s synopsis of psychiatry (12th ed.). Wolters Kluwer.
Bolton, D. (2022). The biopsychosocial model: Its implementation in psychiatry and its status as a scientific theory. In D. Stein & N. Bhagwanjee (Eds.), Biopsychosocial factors in psychiatry (pp. 3–24). Oxford University Press.
Carlat, D. J. (2024). The psychiatric interview (5th ed.). Wolters Kluwer.
Carter, R. T., Kirkinis, K., & Johnson, V. E. (2022). Relationships between trauma symptoms and race–based traumatic stress. Traumatology, 28(1), 11–22. https://doi.org/10.1037/trm0000217
Mullins, N., & Lewis, C. M. (2023). Genetics of bipolar disorder and major depressive disorder. In M. J. Owen & M. C. O’Donovan (Eds.), Psychiatric genetics. Cambridge University Press. https://doi.org/10.1017/9781108617420
Cowan, H. R., Lundin, N. B., Moe, A. M., & Breitborde, N. J. K. (2023). Expressed emotion, human agency, and schizophrenia: Toward a new model for the EE–relapse association. Journal of Psychiatric Research, 162, 220–227. https://doi.org/10.1016/j.jpsychires.2023.05.035
Corrigan, P. W., Bink, A. B., Schmidt, A., Jones, N., & Rüsch, N. (2022). What is the impact of self–stigma? Loss of self–respect and the ‘why try’ effect. Journal of Mental Health, 25(1), 10–15.
Cross-Disorder Group of the Psychiatric Genomics Consortium. (2022). Genomic relationships, novel loci, and pleiotropic mechanisms across eight psychiatric disorders. Cell, 179(7), 1469–1482. https://doi.org/10.1016/j.cell.2019.11.020
Cuthbert, B. N. (2022). Research Domain Criteria: Toward future psychiatric nosologies. Dialogues in Clinical Neuroscience, 17(1), 89–97. https://doi.org/10.31887/DCNS.2015.17.1/bcuthbert
Eisenberger, N. I., & Moieni, M. (2023). Inflammation affects social experience: Implications for mental health. World Psychiatry, 19(2), 121–132. https://doi.org/10.1002/wps.20724
McKay, M. T., Kilmartin, L., Meagher, A., Cannon, M., Healy, C., & Clarke, M. C. (2022). A revised and extended systematic review and meta–analysis of the relationship between childhood adversity and adult psychiatric disorder. Journal of Psychiatric Research, 156, 268–283. https://doi.org/10.1016/j.jpsychires.2022.09.042
Grotzinger, A. D., Mallard, T. T., Akingbuwa, W. A., et al. (2022). Genetic architecture of 11 major psychiatric disorders at biobehavioral, functional genomic and molecular genetic levels of analysis. Nature Genetics, 54(5), 548–559. https://doi.org/10.1038/s41588-022-01057-4
Carmassi, C., Conti, L., Gravina, D., Nardi, B., & Dell’Osso, L. (2022). Emotional dysregulation as a trans–nosographic psychopathological dimension in adulthood: A systematic review. Frontiers in Psychiatry, 13, 900277. https://doi.org/10.3389/fpsyt.2022.900277
Shadrina, M., Bondarenko, E. A., & Slominsky, P. A. (2024). Genetics factors in major depression disorder. Frontiers in Psychiatry, 9, 334. https://doi.org/10.3389/fpsyt.2018.00334), 444–454.
Kirmayer, L. J., Jarvis, G. E., & Guzder, J. (2022). Cultural consultation: Encountering the other in clinical practice. In L. J. Kirmayer & N. Sartorius (Eds.), Cultural formulation: A reader for psychiatric diagnosis (2nd ed.). Springer.
Lupien, S. J., Juster, R. P., Raymond, C., & Marin, M. F. (2022). The effects of chronic stress on the human brain: From neurotoxicity to vulnerability. Frontiers in Neuroendocrinology, 49, 91–105. https://doi.org/10.1016/j.yfrne.2022.100_lupien
Starks, T. J., Sauermilch, D., Grov, C., & Parsons, J. T. (2021). Cannabis use and psychosis: Updated systematic review and meta–analysis. Psychological Medicine, 51(13), 2138–2150. https://doi.org/10.1017/S0033291721002816
McEwen, B. S., & Akil, H. (2023). Revisiting the stress concept: Implications for affective disorders. Journal of Neuroscience, 40(1), 12–21. https://doi.org/10.1523/JNEUROSCI.0733-19.2019
Cowan, C. S. M., Callaghan, B. L., Kan, J. M., & Richardson, R. (2021). The lasting impact of early–life adversity on individuals and their descendants: Potential mechanisms and hope for intervention. Genes, Brain and Behavior, 16(1), 134–151. https://doi.org/10.1111/gbb.12407
McLaughlin, K. A., Colich, N. L., Rodman, A. M., & Weissman, D. G. (2021). Mechanisms linking childhood trauma exposure and psychopathology: A transdiagnostic model of risk and resilience. BMC Medicine, 19, 96. https://doi.org/10.1186/s12916-021-01920-3
Mikulincer, M., & Shaver, P. R. (2022). An attachment perspective on psychopathology. World Psychiatry, 21(2), 171–187. https://doi.org/10.1002/wps.20971
Pruessner, M., Cullen, A. E., Aas, M., & Walker, E. F. (2023). The diathesis–stress model of schizophrenia: An update and extended discussion. Schizophrenia Bulletin, 49(3), 532–549. https://doi.org/10.1093/schbul/sbac204
Kirkbride, J. B., Anglin, D. M., Colman, I., Dykxhoorn, J., Jones, P. B., Patalay, P., Pitman, A., Soneson, E., Steare, T., Wright, T., & Griffiths, S. L. (2024). The social determinants of mental health and disorder: Evidence, prevention and recommendations. World Psychiatry, 23(1), 58–90. https://doi.org/10.1002/wps.21160
Zuckerman, M., & Knee, C. R. (2023). Psychobiological models of personality and psychopathology: Diathesis–stress and beyond. Annual Review of Clinical Psychology, 19, 63–88. https://doi.org/10.1146/annurev-clinpsy-2023
Lund, C., Brooke-Sumner, C., Baingana, F., Baron, E. C., Breuer, E., Chandra, P., Haushofer, J., Herrman, H., Jordans, M., Kieling, C., Medina-Mora, M. E., Morgan, E., Ormel, J., Plunkett, H., Saxena, S., Thornicroft, G., Thornicroft, G., Yasamy, M. T., & Patel, V. (2022). Social determinants of mental disorders and the Sustainable Development Goals: A systematic review of reviews. The Lancet Psychiatry, 9(1), 85–95. https://doi.org/10.1016/S2215-0366(21)00355-4
Selten, J. P., van der Ven, E., & Termorshuizen, F. (2021). Social defeat theory of schizophrenia: An update. Schizophrenia Research, 228, 77–83. https://doi.org/10.1016/j.schres.2021.01.001
Seligman, M. E. P. (2022). Learned helplessness, learned optimism, and the controllability of life events. Frontiers in Psychology, 13, 1038822. https://doi.org/10.3389/fpsyg.2022.1038822
Wade, M., Zeanah, C. H., Fox, N. A., & Nelson, C. A. (2021). Stress sensitization as a mediator of the relationship between early institutional deprivation and internalizing symptoms in adolescence. JAMA Psychiatry, 78(2), 186–194. https://doi.org/10.1001/jamapsychiatry.2020.3273
Solmi, M., Radua, J., Olivola, M., et al. (2022). Age at onset of mental disorders worldwide: Large–scale meta–analysis of 192 epidemiological studies. Molecular Psychiatry, 27(1), 281–295.
Sonuga-Barke, E. J. S., Kennedy, M., Golm, D., Knights, N., Kovshoff, H., Kumsta, R., Schlotz, W., Stevens, S., Straatman, H., & Kreppner, J. (2023). Long–term effects of early childhood institutional deprivation on adolescent mental health: The English and Romanian Adoptees study. The Lancet Psychiatry, 10(5), 341–350. https://doi.org/10.1016/S2215-0366(23)00059-0
Murray, G. K., Lin, T., Austin, J., McGrath, J. J., Hickie, I. B., & Wray, N. R. (2021). Could polygenic risk scores be useful in psychiatry?: A review. JAMA Psychiatry, 78(2), 210–219. https://doi.org/10.1001/jamapsychiatry.2020.3042
Cowan, C. S. M., Callaghan, B. L., Kan, J. M., & Richardson, R. (2021). The lasting impact of early–life adversity on individuals and their descendants: Potential mechanisms and hope for intervention. Genes, Brain and Behavior, 16(1), 134–151. https://doi.org/10.1111/gbb.12407
van Os, J., Guloksuz, S., Vijn, T. W., Hafkenscheid, A., & Delespaul, P. (2022). The evidence–based group–level symptom–reduction model as the organizing principle for mental health care: Time for change? World Psychiatry, 18(1), 88–96. https://doi.org/10.1002/wps.20609
Williams, D. R., Lawrence, J. A., Davis, B. A., & Vu, C. (2024). Understanding how discrimination can affect health. Health Services Research, 54(S2), 1374–1388. https://doi.org/10.1111/1475-6773.13222
Yehuda, R., Lehrner, A., & Rosenbaum, T. Y. (2021). PTSD and sexual dysfunction in men and women. Journal of Sexual Medicine, 12(5), 1107–1119. https://doi.org/10.1002/wps.21073
About the Author
Dan Palmer is a psychiatric–mental health nursing professional with clinical expertise spanning inpatient psychiatric settings, outpatient community mental health, and substance use disorder treatment. He holds advanced practice training in psychopathology, diagnostic reasoning, and evidence–based psychiatric treatment, and has supported PMHNP students at Walden University and across online nursing programs in developing the clinical reasoning skills that bridge graduate coursework and real–world practice.
Dan writes from the conviction that the best PMHNP education does not separate clinical science from clinical humanity. His content integrates current neuroscience, evidence–based psychological frameworks, and the realities of practicing in a healthcare system where social determinants of health shape outcomes as powerfully as pharmacology. He is particularly focused on helping PMHNP students develop the integrative biopsychosocial reasoning that distinguishes advanced practice from algorithmic prescription.
Connect with Dan on LinkedIn: linkedin.com/in/dan-palmer–a49378108